

Successful pregnancy and live birth from a hypogonadotropic hypogonadism woman with low serum estradiol concentrations despite numerous oocyte maturations: a case report
- PMID: 28931393
- PMCID: PMC5607600
- DOI: 10.1186/s12884-017-1510-6
Successful pregnancy and live birth from a hypogonadotropic hypogonadism woman with low serum estradiol concentrations despite numerous oocyte maturations: a case report
Abstract
Background: The increase in serum estradiol (E2) concentrations during the follicular phase becomes the index of oocyte maturation in vivo. When ovarian stimulation is performed to hypogonadotropic hypogonadism (HH) patients with only follicle stimulating hormone (FSH), proper increase in serum E2 concentrations is not observed. Even if oocytes are obtained, which usually have low fertilization rate. In this report, we would like to present an unique case, in which under low E2 concentrations and without luteinizing hormone (LH) administration, numerous mature oocytes could be obtained and a healthy baby delivered.
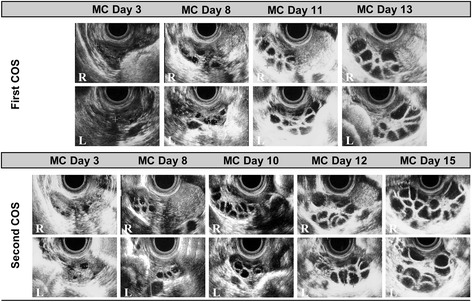
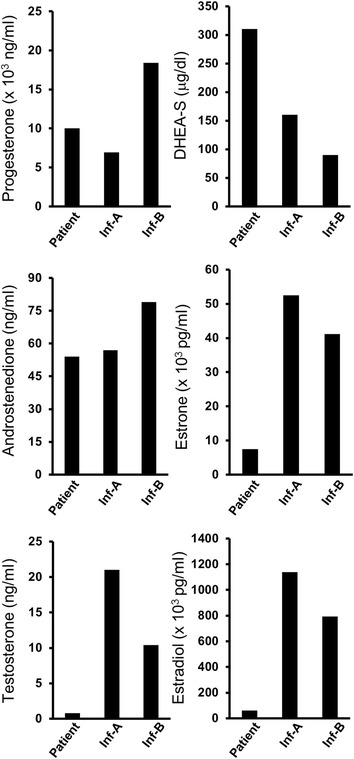
Case presentation: During controlled ovarian stimulation (COS) with only recombinant follicular stimulating hormone (rFSH) administrations, a 26-year-old Japanese woman with hypothalamic amenorrhea (i.e., hypogonadotropic hypogonadism) developed numerous follicles despite low serum E2, 701 pg/ml, and high progesterone (P4) concentrations, 2.11 ng/ml, on the day of induced ovulation. However, 33 cumulus-oocyte complexes (COCs) were successfully obtained; following the embryo culture, four early embryos and six blastocysts were cryopreserved. This patient received hormone replacement therapy (HRT), during which one of six cryopreserved blastocysts was thawed and transferred into the uterine lumen. The patient became pregnant from the first transfer, went through her pregnancy without any complications, and delivered a healthy male baby in the 39th week. Low E2 concentrations in follicular fluids (FFs) are suggestive that aromatase and/or 17β-hydroxysteroid dehydrogenase (17β-HSD) could be low.
Conclusions: Serum E2 concentrations may not be the most important index for oocyte maturation during COS, and suggested that oocyte maturation was in progress even under low serum E2 and high P4 conditions. Even if serum E2 concentrations did not properly increase, numerous mature oocytes could be obtained, resulting in the birth of a healthy baby.
Keywords: Assisted reproductive technology; Controlled ovarian stimulation; Follicular fluids; High progesterone; Hypogonadotropic hypogonadism; Hypothalamic amenorrhea; Low estradiol; Luteinizing hormone.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any images and clinical data. A copy of the written consent is available for reviewer by the editor of this journal.
Competing interests
All the author’s declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
[Effect of bushen tiaojing recipe on the quality of the oocytes and reproductive hormones in the follicular fluid in IVF-ET patients].Zhongguo Zhong Xi Yi Jie He Za Zhi. 2014 Aug;34(8):911-6. Zhongguo Zhong Xi Yi Jie He Za Zhi. 2014. PMID: 25223171 Clinical Trial. Chinese.
-
Relationship between follicular volume and oocyte competence, blastocyst development and live-birth rate: optimal follicle size for oocyte retrieval.Ultrasound Obstet Gynecol. 2018 Jan;51(1):118-125. doi: 10.1002/uog.18955. Ultrasound Obstet Gynecol. 2018. PMID: 29134715
-
Intrafollicular content of luteinizing hormone receptor, alpha-inhibin, and aromatase in relation to follicular growth, estrous cycle stage, and oocyte competence for in vitro maturation in the mare.Biol Reprod. 1999 May;60(5):1120-7. doi: 10.1095/biolreprod60.5.1120. Biol Reprod. 1999. PMID: 10208973
-
Ovarian follicular and luteal physiology.Int Rev Physiol. 1980;22:117-201. Int Rev Physiol. 1980. PMID: 6248477 Review.
-
Pregnancy despite imminent ovarian failure and extremely high endogenous gonadotropins and therapeutic strategies: case report and review.Clin Exp Obstet Gynecol. 2004;31(4):299-301. Clin Exp Obstet Gynecol. 2004. PMID: 15672973 Review.
References
-
- Erickson GF. An analysis of follicle development and ovum maturation. Semin Reprod Med. 1986;4(3):233–254. doi: 10.1055/s-2007-1022504. - DOI
-
- Balasch J, Miró F, Burzaco I, Casamitjana R, Civico S, Ballescá JL, et al. The role of luteinizing hormone in human follicle development and oocyte fertility: evidence from in-vitro fertilization in a woman with long-standing hypogonadotrophic hypogonadism and using recombinant human follicle stimulating hormone. Hum Reprod. 1995;10(7):1678–1683. doi: 10.1093/oxfordjournals.humrep.a136154. - DOI - PubMed
-
- The European Recombinant Human LH Study Group Recombinant human luteinizing hormone (LH) to support recombinant human follicle-stimulating hormone (FSH)-induced follicular development in LH- and FSH-deficient anovulatory women: a dose-finding study. J Clin Endocrinol Metab. 1998;83(5):1507–1514. - PubMed
-
- World Health Organization . WHO laboratory manual for the examination and processing of human semen. 5. Geneva: WHO; 2010. Department of Reproductive Health and Research.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
