

A step-by-step guide to office-based sperm retrieval for obstructive azoospermia
- PMID: 28904906
- PMCID: PMC5583054
- DOI: 10.21037/tau.2017.07.15
A step-by-step guide to office-based sperm retrieval for obstructive azoospermia
Abstract
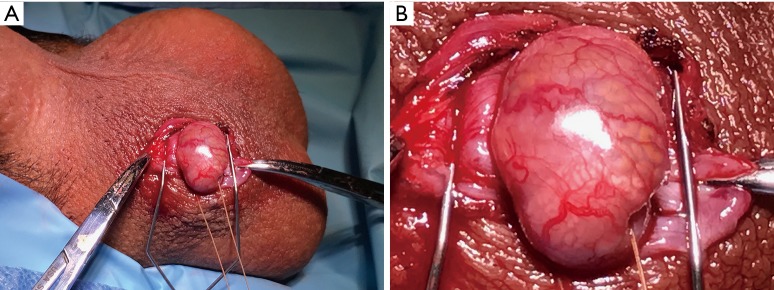
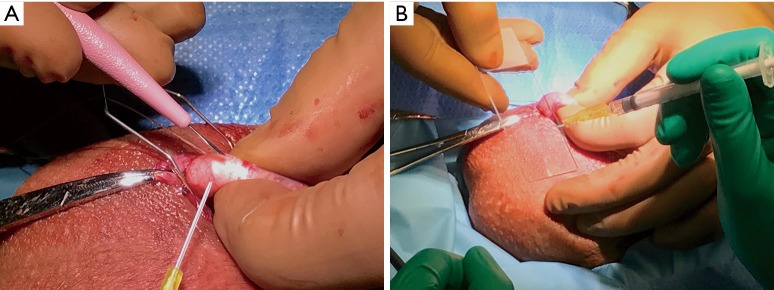
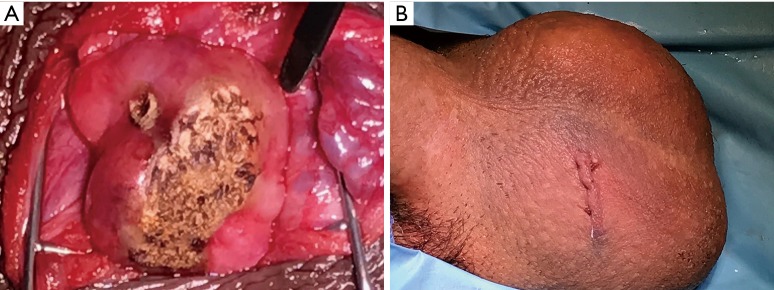
A variety of surgical options exists for sperm retrieval in the setting of obstructive azoospermia (OA). With appropriate preparation, the majority of these techniques can safely be performed in the office with local anesthesia and with or without monitored anesthesia care (MAC). The available techniques include percutaneous options such as percutaneous epididymal sperm aspiration (PESA) and testicular sperm aspiration (TESA), as well as open techniques that include testicular sperm extraction (TESE) and microsurgical epididymal sperm aspiration (MESA). In addition to providing a step-by-step description of each available approach, we introduce and describe a new technique for sperm retrieval for OA called minimally invasive epididymal sperm aspiration (MIESA). The MIESA utilizes a tiny keyhole incision, and the epididymis is exposed without testicular delivery. Epididymal aspiration is performed in the style of MESA, except using loupe magnification rather than an operating microscope. MIESA is a safe, office-based procedure in which millions of motile sperm can be retrieved for cryopreservation. While we prefer the MIESA technique for OA, there remain distinct advantages of each open and percutaneous approach. In the current era of assisted reproductive technology, sperm retrieval rates for OA should approach 100% regardless of the technique. This reference provides a roadmap for both advanced and novice male reproductive surgeons to guide them through every stage of sperm retrieval for OA, including preoperative evaluation, patient selection, procedural techniques, and complications. With the incredible advances in in vitro fertilization (IVF), combined with innovative surgical treatment for male factor infertility in recent years, OA is no longer a barrier for men to become biologic fathers.
Keywords: MESA; MIESA; Obstructive azoospermia (OA); PESA; TESA; TESE; epididymal sperm; sperm retrieval; testicular sperm.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Percutaneous epididymal sperm aspiration versus microsurgical epididymal sperm aspiration for irreparable obstructive azoospermia--experience with 100 cases.J Formos Med Assoc. 2000 Jun;99(6):459-65. J Formos Med Assoc. 2000. PMID: 10925551
-
Outcome of in vitro fertilization and intracytoplasmic injection of epididymal and testicular sperm obtained from patients with obstructive and nonobstructive azoospermia.J Urol. 2002 Apr;167(4):1753-6. J Urol. 2002. PMID: 11912403
-
Open epididymal sperm aspiration (OESA): minimally invasive surgical technique for sperm retrieval.Arch Esp Urol. 2006 Apr;59(3):313-6. doi: 10.4321/s0004-06142006000300020. Arch Esp Urol. 2006. PMID: 16724722
-
[Operative sperm retrieval - the urological aspects].Urologe A. 1999 Nov;38(6):563-8. doi: 10.1007/s001200050328. Urologe A. 1999. PMID: 10591801 Review. German.
-
Techniques for surgical retrieval of sperm prior to ICSI for azoospermia.Cochrane Database Syst Rev. 2001;(4):CD002807. doi: 10.1002/14651858.CD002807. Cochrane Database Syst Rev. 2001. Update in: Cochrane Database Syst Rev. 2006 Jul 19;(3):CD002807. doi: 10.1002/14651858.CD002807.pub2. PMID: 11687162 Updated. Review.
Cited by
-
Male infertility due to testicular disorders.J Clin Endocrinol Metab. 2021 Jan 23;106(2):e442-e459. doi: 10.1210/clinem/dgaa781. J Clin Endocrinol Metab. 2021. PMID: 33295608 Free PMC article. Review.
-
Testicular sperm aspiration has a poor effect in predicting micro-TESE outcomes in NOA patients with AZFc deletion.Basic Clin Androl. 2023 Aug 10;33(1):28. doi: 10.1186/s12610-023-00195-x. Basic Clin Androl. 2023. PMID: 37558984 Free PMC article.
-
[Desire to have children after vasectomy : Vasectomy reversal or assisted reproductive technology?].Urologie. 2024 Nov;63(11):1111-1121. doi: 10.1007/s00120-024-02454-9. Epub 2024 Oct 16. Urologie. 2024. PMID: 39414715 German.
-
Pregnancy outcomes in patients with non-obstructive azoospermia undergoing micro-TESE: comparison of fresh vs. frozen-thawed testicular sperm.J Assist Reprod Genet. 2024 Dec;41(12):3399-3404. doi: 10.1007/s10815-024-03291-7. Epub 2024 Oct 21. J Assist Reprod Genet. 2024. PMID: 39432191
-
Bridging the Gap: Animal Models in Next-Generation Reproductive Technologies for Male Fertility Preservation.Life (Basel). 2023 Dec 21;14(1):17. doi: 10.3390/life14010017. Life (Basel). 2023. PMID: 38276265 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources