

Comprehensive geriatric assessment for older adults admitted to hospital
- PMID: 28898390
- PMCID: PMC6484374
- DOI: 10.1002/14651858.CD006211.pub3
Comprehensive geriatric assessment for older adults admitted to hospital
Abstract
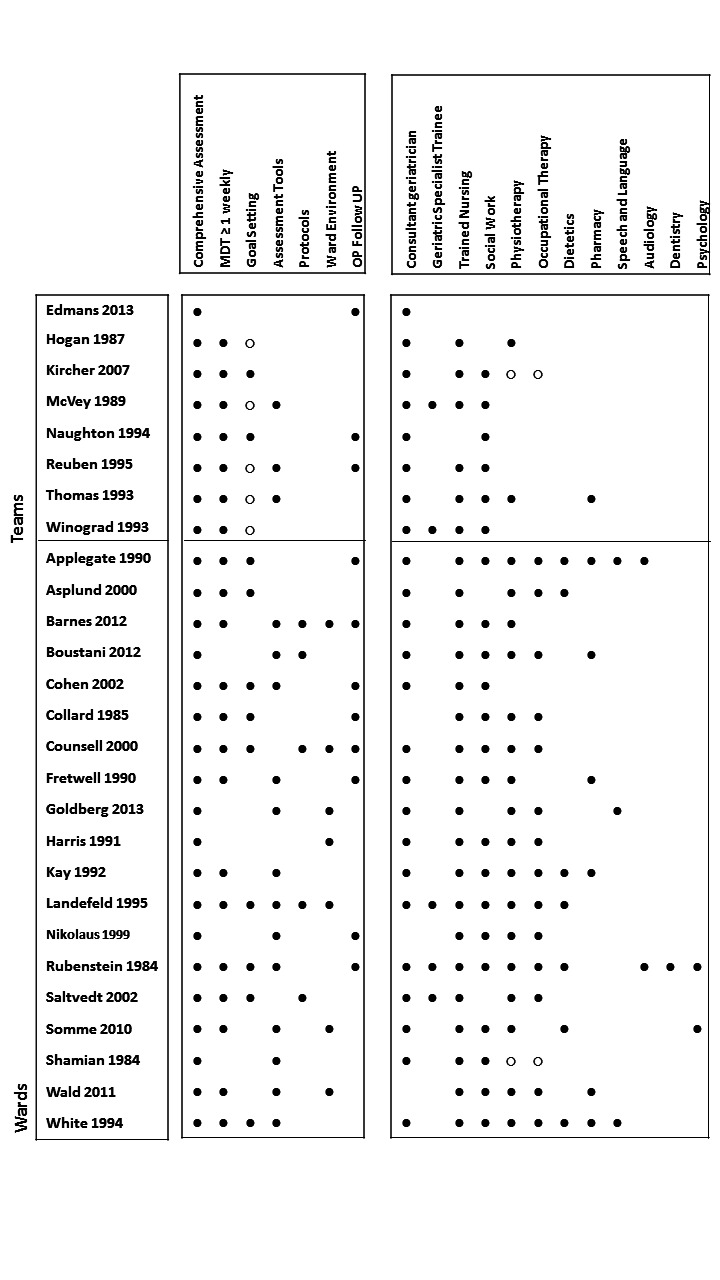
Background: Comprehensive geriatric assessment (CGA) is a multi-dimensional, multi-disciplinary diagnostic and therapeutic process conducted to determine the medical, mental, and functional problems of older people with frailty so that a co-ordinated and integrated plan for treatment and follow-up can be developed. This is an update of a previously published Cochrane review.
Objectives: We sought to critically appraise and summarise current evidence on the effectiveness and resource use of CGA for older adults admitted to hospital, and to use these data to estimate its cost-effectiveness.
Search methods: We searched CENTRAL, MEDLINE, Embase, three other databases, and two trials registers on 5 October 2016; we also checked reference lists and contacted study authors.
Selection criteria: We included randomised trials that compared inpatient CGA (delivered on geriatric wards or by mobile teams) versus usual care on a general medical ward or on a ward for older people, usually admitted to hospital for acute care or for inpatient rehabilitation after an acute admission.
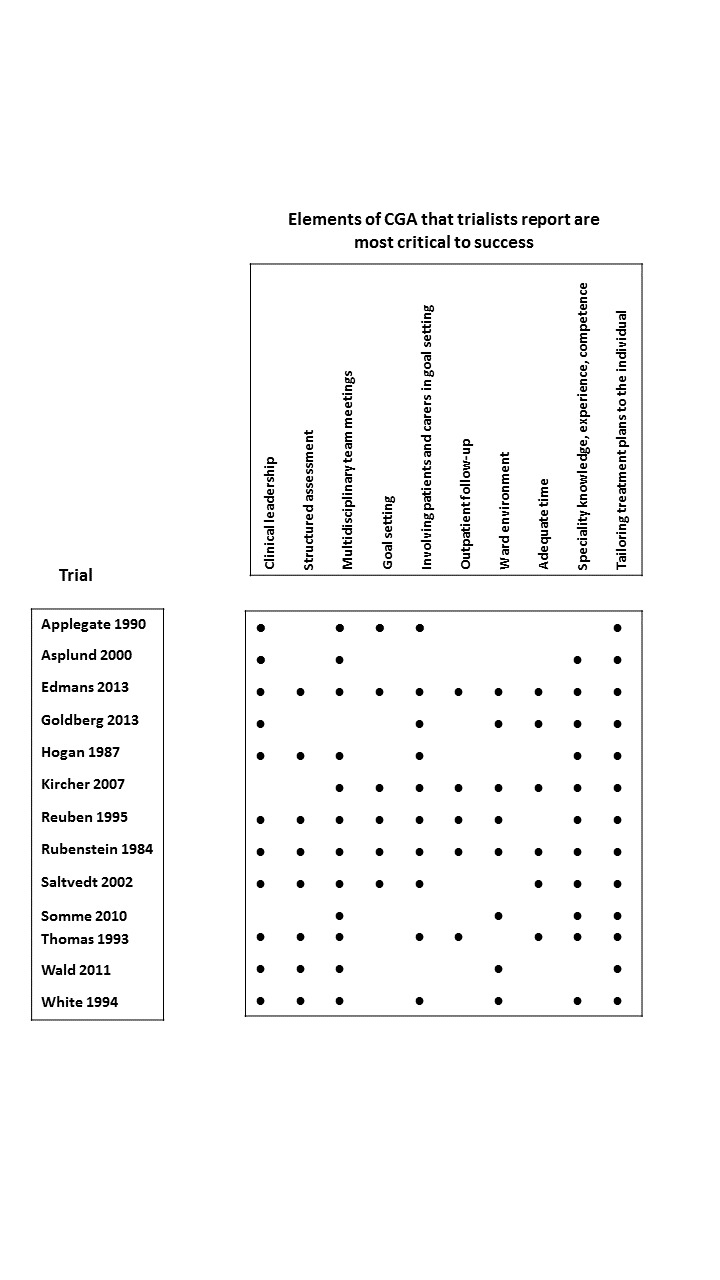
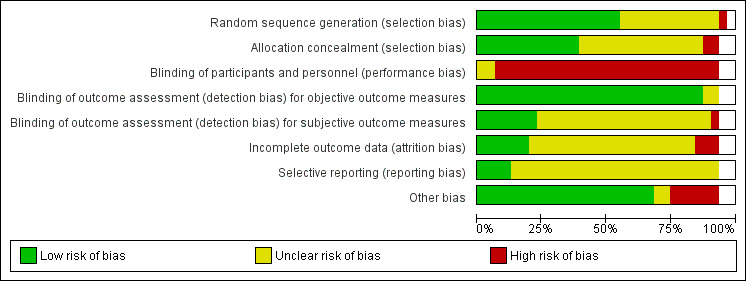
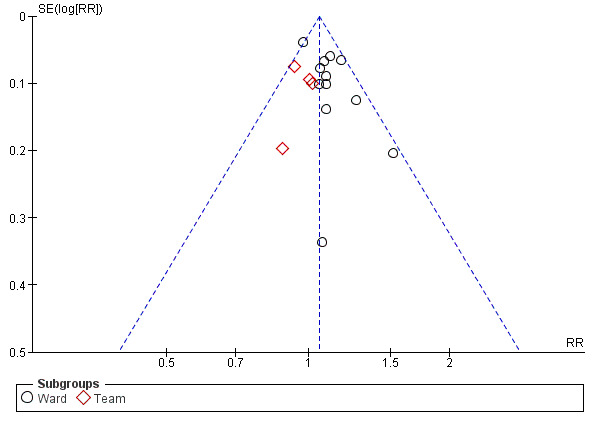
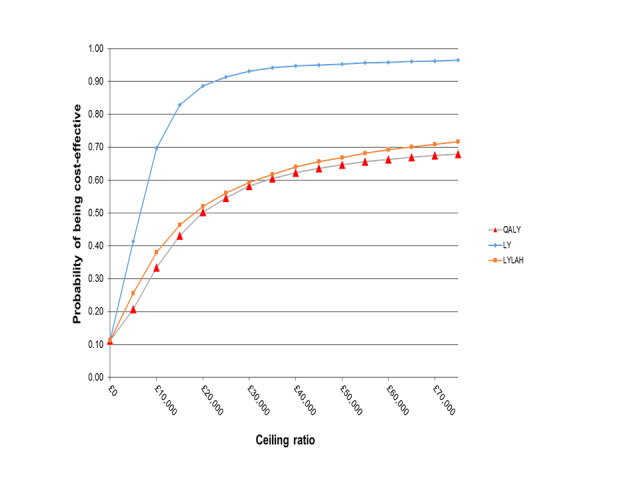
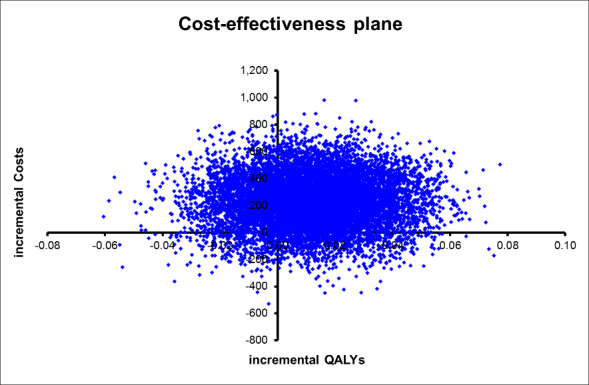
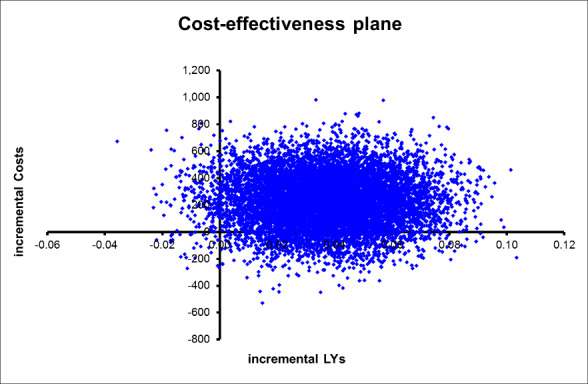
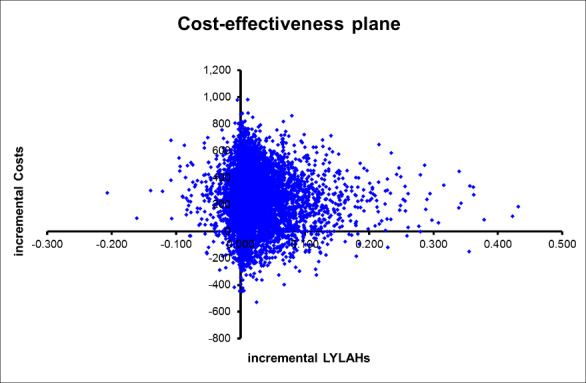
Data collection and analysis: We followed standard methodological procedures expected by Cochrane and Effective Practice and Organisation of Care (EPOC). We used the GRADE approach to assess the certainty of evidence for the most important outcomes. For this update, we requested individual patient data (IPD) from trialists, and we conducted a survey of trialists to obtain details of delivery of CGA. We calculated risk ratios (RRs), mean differences (MDs), or standardised mean differences (SMDs), and combined data using fixed-effect meta-analysis. We estimated cost-effectiveness by comparing inpatient CGA versus hospital admission without CGA in terms of cost per quality-adjusted life year (QALY) gained, cost per life year (LY) gained, and cost per life year living at home (LYLAH) gained.
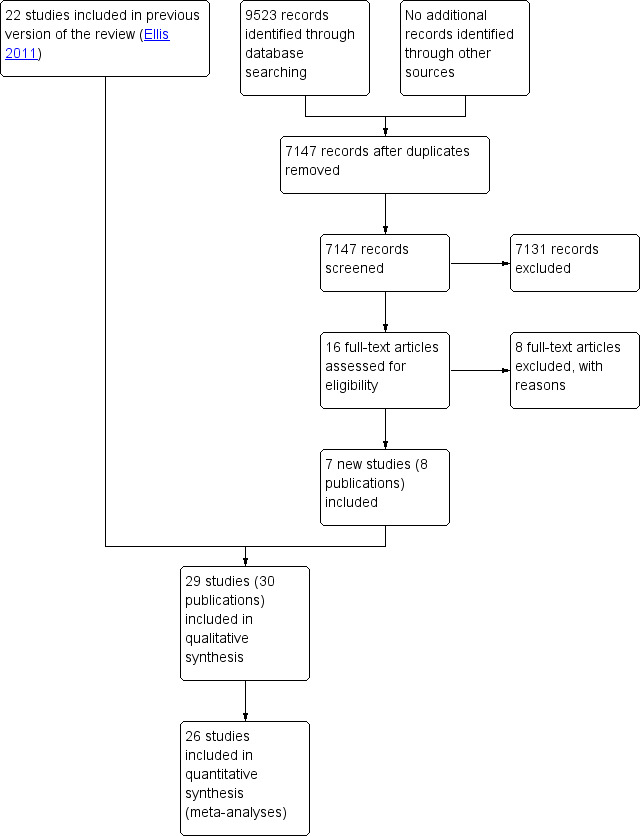
Main results: We included 29 trials recruiting 13,766 participants across nine, mostly high-income countries. CGA increases the likelihood that patients will be alive and in their own homes at 3 to 12 months' follow-up (risk ratio (RR) 1.06, 95% confidence interval (CI) 1.01 to 1.10; 16 trials, 6799 participants; high-certainty evidence), results in little or no difference in mortality at 3 to 12 months' follow-up (RR 1.00, 95% CI 0.93 to 1.07; 21 trials, 10,023 participants; high-certainty evidence), decreases the likelihood that patients will be admitted to a nursing home at 3 to 12 months follow-up (RR 0.80, 95% CI 0.72 to 0.89; 14 trials, 6285 participants; high-certainty evidence) and results in little or no difference in dependence (RR 0.97, 95% CI 0.89 to 1.04; 14 trials, 6551 participants; high-certainty evidence). CGA may make little or no difference to cognitive function (SMD ranged from -0.22 to 0.35 (5 trials, 3534 participants; low-certainty evidence)). Mean length of stay ranged from 1.63 days to 40.7 days in the intervention group, and ranged from 1.8 days to 42.8 days in the comparison group. Healthcare costs per participant in the CGA group were on average GBP 234 (95% CI GBP -144 to GBP 605) higher than in the usual care group (17 trials, 5303 participants; low-certainty evidence). CGA may lead to a slight increase in QALYs of 0.012 (95% CI -0.024 to 0.048) at GBP 19,802 per QALY gained (3 trials; low-certainty evidence), a slight increase in LYs of 0.037 (95% CI 0.001 to 0.073), at GBP 6305 per LY gained (4 trials; low-certainty evidence), and a slight increase in LYLAH of 0.019 (95% CI -0.019 to 0.155) at GBP 12,568 per LYLAH gained (2 trials; low-certainty evidence). The probability that CGA would be cost-effective at a GBP 20,000 ceiling ratio for QALY, LY, and LYLAH was 0.50, 0.89, and 0.47, respectively (17 trials, 5303 participants; low-certainty evidence).
Authors' conclusions: Older patients are more likely to be alive and in their own homes at follow-up if they received CGA on admission to hospital. We are uncertain whether data show a difference in effect between wards and teams, as this analysis was underpowered. CGA may lead to a small increase in costs, and evidence for cost-effectiveness is of low-certainty due to imprecision and inconsistency among studies. Further research that reports cost estimates that are setting-specific across different sectors of care are required.
Conflict of interest statement
Graham Ellis: none known.
Mike Gardner: none known.
Apostolos Tsiachristas: none known.
Peter Langhorne: none known.
Orlaith Burke: none known.
Rowan H Harwood: trialist.
Simon P Conroy: trialist.
Tilo Kircher: trialist.
Dominique Somme: trialist.
Ingvild Saltvedt: trialist.
Heidi Wald: trialist.
Desmond O'Neill: none known.
David Robinson: none known.
Sasha Shepperd: none known.
Figures












Update of
-
Comprehensive geriatric assessment for older adults admitted to hospital.Cochrane Database Syst Rev. 2011 Jul 6;(7):CD006211. doi: 10.1002/14651858.CD006211.pub2. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2017 Sep 12;9:CD006211. doi: 10.1002/14651858.CD006211.pub3. PMID: 21735403 Free PMC article. Updated. Review.
Similar articles
-
Comprehensive Geriatric Assessment for community-dwelling, high-risk, frail, older people.Cochrane Database Syst Rev. 2022 May 6;5(5):CD012705. doi: 10.1002/14651858.CD012705.pub2. Cochrane Database Syst Rev. 2022. PMID: 35521829 Free PMC article. Review.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Comprehensive geriatric assessment for older adults admitted to hospital.Cochrane Database Syst Rev. 2011 Jul 6;(7):CD006211. doi: 10.1002/14651858.CD006211.pub2. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2017 Sep 12;9:CD006211. doi: 10.1002/14651858.CD006211.pub3. PMID: 21735403 Free PMC article. Updated. Review.
-
Case management for integrated care of older people with frailty in community settings.Cochrane Database Syst Rev. 2023 May 23;5(5):CD013088. doi: 10.1002/14651858.CD013088.pub2. Cochrane Database Syst Rev. 2023. PMID: 37218645 Free PMC article. Review.
-
Early discharge hospital at home.Cochrane Database Syst Rev. 2017 Jun 26;6(6):CD000356. doi: 10.1002/14651858.CD000356.pub4. Cochrane Database Syst Rev. 2017. PMID: 28651296 Free PMC article. Review.
Cited by
-
E-Health-based, trans-sectoral, geriatric health service - Geriatric Network (GerNe).Sci Rep. 2024 Jul 27;14(1):17326. doi: 10.1038/s41598-024-67624-3. Sci Rep. 2024. PMID: 39068175 Free PMC article.
-
Acute frailty services: results of a national day of care survey.BMC Geriatr. 2024 Jul 16;24(1):608. doi: 10.1186/s12877-024-05075-1. BMC Geriatr. 2024. PMID: 39014306 Free PMC article.
-
Early Supported Discharge for Older Adults Admitted to Hospital with Medical Complaints: A Qualitative Study Exploring the Views of Stakeholders.J Multidiscip Healthc. 2022 Dec 16;15:2861-2870. doi: 10.2147/JMDH.S380572. eCollection 2022. J Multidiscip Healthc. 2022. PMID: 36561433 Free PMC article.
-
Resilience in Clinical Care: Getting a Grip on the Recovery Potential of Older Adults.J Am Geriatr Soc. 2019 Dec;67(12):2650-2657. doi: 10.1111/jgs.16149. Epub 2019 Sep 9. J Am Geriatr Soc. 2019. PMID: 31498881 Free PMC article. Review.
-
Prevalence and implications of frailty in acute stroke: systematic review & meta-analysis.Age Ageing. 2022 Mar 1;51(3):afac064. doi: 10.1093/ageing/afac064. Age Ageing. 2022. PMID: 35352795 Free PMC article.
References
References to studies included in this review
Applegate 1990 {published data only}
-
- Applegate WB, Miller ST, Graney MJ, Elam JT, Burns R, Akins DE. A randomized, controlled trial of a geriatric assessment unit in a community rehabilitation hospital. New England Journal of Medicine 1990;322:1572‐8. - PubMed
-
- Miller ST, Applegate WB, Elam JT, Graney MJ. Influence of diagnostic classification on outcomes and charges in geriatric assessment and rehabilitation. Journal of the American Geriatrics Society 1994;42:11‐5. - PubMed
Asplund 2000 {published data only}
-
- Asplund K, Gustafsen Y, Jacobsson C, Bucht G, Wahlin A, Peterson J, et al. Geriatric‐based versus general wards for older acute medical patients: a randomised comparison of outcomes and use of resources. Journal of the American Geriatrics Society 2000;48:1381‐8. - PubMed
Barnes 2012 {published and unpublished data}
Boustani 2012 {published and unpublished data}
Cohen 2002 GEMC {published data only}
-
- Cohen HJ, Feussner JR, Weinberger M, Carnes M, Hamdy RC, Hsieh F, et al. A controlled trial of inpatient and outpatient geriatric evaluation and management. New England Journal of Medicine 2002;346:905‐12. - PubMed
Cohen 2002 UCOP {published data only}
-
- Cohen HJ, Feussner JR, Weinberger M, Carnes M, Hamdy RC, Hsieh F, et al. A controlled trial of inpatient and outpatient geriatric evaluation and management. New England Journal of Medicine 2002;346:905‐12. - PubMed
Collard 1985 {published data only}
-
- Bachman SS, Collard AF, Greenberg JN, Fountain E, Huebner TW, Kimball B, et al. An innovative approach to geriatric acute care delivery: the Choate‐Symmes experience. Hospital & Health Services Administration 1987;November:509‐20. - PubMed
-
- Collard AF, Bachman SS, Beatrice DF. Acute care delivery for the geriatric patient: an innovative approach. Quarterly Review Bulletin 1985;June:180‐5. - PubMed
Counsell 2000 {published data only}
-
- Counsell SR, Holder CM, Liebenauer LL, Palmer RM, Fortinsky RH, Kresevic DM, et al. Effects of a multicomponent intervention on functional outcomes and process of care in hospitalised older patients: a randomised controlled trial of acute care for elders (ACE) in a community hospital. Journal of the American Geriatrics Society 2000;48:1572‐81. - PubMed
Edmans 2013 {published and unpublished data}
-
- Tanajewski L, Franklin M, Gkoutouras G, Berdunov V, Edmans J, Conroy S, et al. Cost‐effectiveness of a specialist geriatric medical intervention for frail older people discharged from acute medical units: economical evaluation in a two‐centre randomised controlled trial (AMIGOS). PLOS ONE 2015;10(5):doi:10.1371/journal. - PMC - PubMed
Fretwell 1990 {published data only}
-
- Fretwell MD, Raymond PM, McGarvey ST, Owens N, Traines M, Silliman RA, et al. The senior care study. A controlled trial of a consultative / unit based geriatric assessment program in acute care. Journal of the American Geriatrics Society 1990;38:1073‐81. - PubMed
-
- Silliman RA, McGarvey ST, Raymond PM, Fretwell MD. Senior care study: does inpatient interdisciplinary geriatric assessment help the family caregivers of acutely ill older patients?. Journal of the American Geriatrics Society 1990;38(4):461‐6. - PubMed
Goldberg 2013 {published and unpublished data}
-
- Goldberg SE, Bradshaw LE, Kearney FC, Russell C, Whittamore KH, Foster PER, et al. Care in specialist medical and mental health unit compared with standard care for older people with cognitive impairment admitted to general hospital: randomised controlled trial (NIHR TEAM trial). BMJ 2013;347:doi: 10.1136/bmj.f4132. - PMC - PubMed
Harris 1991 {published data only}
-
- Harris RD, Henschke PJ, Popplewell PY, Radford AJ, Bond MJ, Turnbull RJ, et al. A randomised study of outcomes in a defined group of acutely ill elderly patients managed in a geriatric assessment unit or a general medical unit. Australian and New Zealand Journal of Medicine 1991;21:230‐4. - PubMed
Hogan 1987 {published data only}
Kay 1992 {published data only}
-
- Kay G, MacTavish M, Moffat C, Lau G. Development and evaluation of a geriatric assessment unit in a community hospital. Fall 1992;16(3):2‐9. - PubMed
Kircher 2007 {published data only}
-
- Kircher TJ, Wormstall H, Muller PH, Schwarzler F, Buchkremer G, Wild K, et al. A randomised trial of a geriatric evaluation and management consultation services in frail hospitalised patients. Age & Ageing 2007;36:36‐42. [MEDLINE: ] - PubMed
Landefeld 1995 {published data only}
-
- Covinsky KE, King JT, Quinn LM, Siddique R, Palmer R, Kresevic DM, et al. Does acute care for elders units increase hospital costs? A cost analysis using the hospital perspective. Journal of the American Geriatrics Society 1997;45:729‐34. [MEDLINE: ] - PubMed
-
- Covinsky KE, Palmer R, Kresevic DM, Kahana E, Counsell C, Fortinsky RH, et al. Improving functional outcomes in older patients: lessons from an acute care for elders unit. Journal on Quality Improvement 1998;24(2):63‐76. [MEDLINE: ] - PubMed
-
- Landefeld CS, Palmer RM, Krescevic DM, Fortinsky RH, Kowal J. A randomised trial of care in a hospital medical unit especially designed to improve the functional outcomes of acutely ill older patients. New England Journal of Medicine 1995;332:1338‐44. - PubMed
Li 2015 {published and unpublished data}
-
- Li TR, Li Y, Zhang L, Tan AJ. Effects of comprehensive geriatric assessment intervention on Chinese Han older patients with multiple chronic comorbidities. Journal of the American Geriatrics Society 2015;63:S397‐8.
McVey 1989 {published data only}
-
- Allen CA, Becker PM, McVey LJ, Saltz CC, Feussner JR, Cohen HJ. A randomized, controlled clinical trial of a geriatric consultation team. Compliance with recommendations. JAMA 1986;255(19):2617‐21. [MEDLINE: ] - PubMed
-
- Becker PM, McVey LJ, Saltz CC, Feussner JR, Cohen HJ. Hospital‐acquired complications in a randomised controlled clinical trial of a geriatric consultation team. JAMA 1987;17:2313‐7. - PubMed
-
- McVey LJ, Becker PM, Saltz CC, Feussner JR, Cohen HJ. Effect of a geriatric consultation team on functional status of elderly hospitalized patients. Annals of Internal Medicine 1989;110(1):79‐84. [MEDLINE: ] - PubMed
-
- Saltz CC, McVey LJ, Becker PM, Feussner JR, Cohen HJ. Impact of a geriatric consultation team on discharge placement and repeat hospitalization. The Gerontologist 1988;28(3):344‐50. [MEDLINE: ] - PubMed
Naughton 1994 {published data only}
-
- Naughton BJ, Moran MB, Feinglass J, Falconer J, Williams ME. Reducing hospital costs for the geriatric patient admitted from the emergency department: a randomized trial. Journal of the American Geriatrics Society 1994;41:1045‐9. - PubMed
Nikolaus 1999 {published data only}
-
- Nikolaus T, Specht‐Leible N, Bach M, Oster P, Schuerf G. A randomised trial of comprehensive geriatric assessment and home intervention in the care of hospitalised patients. Age & Ageing 1999;28:543‐50. - PubMed
Nikolaus 1999 plus ESD {published data only}
-
- Nikolaus T, Specht‐Leible N, Bach M, Oster P, Schuerf G. A randomised trial of comprehensive geriatric assessment and home intervention in the care of hospitalised patients. Age & Ageing 1999;28:543‐50. - PubMed
Powell 1990 {published data only}
-
- Powell C, Montgomery P. The age study: the admission of geriatric patients through emergency. Age & Ageing 1990;19(Suppl):21‐2. [MEDLINE: ]
Reuben 1995 {published data only}
-
- Reuben DB, Borok GM, Wolde‐Tsadik G, Ershoff DH, Fishman LK, Ambrosini VL, et al. A randomised trial of comprehensive geriatric assessment in the care of hospitalised patients. New England Journal of Medicine 1995;332:1345‐50. - PubMed
Rubenstein 1984 {published data only}
-
- Rubenstein LZ, Josephson KR, Harker JO, Miller DK, Wieland DG. The Sepulveda GEU Study revisited: long‐term outcomes, use of services, and costs. Ageing Clinical & Experimental Research 1995;7:212‐7. [MEDLINE: ] - PubMed
-
- Rubenstein LZ, Josephson KR, Wieland DG, English PA, Sayre JA, Kane RL. Effectiveness of a geriatric evaluation unit. New England Journal of Medicine 1984;311:1664‐70. [MEDLINE: ] - PubMed
-
- Rubenstein LZ, Wieland GD, Josephson KR, Rosbrook B, Sayre J, Kane RL. Improved survival for frail elderly inpatients on a geriatric evaluation unit (GEU): who benefits?. Journal of Clinical Epidemiology 1988;41:441‐9. - PubMed
Saltvedt 2002 {published data only}
-
- Saltvedt I, Jordhoy M, Opdahl Mo ES, Fayers P, Kaasa S, Sletvold O, et al. Randomised trial of in‐hospital geriatric intervention: impact on function and morale [Sletvold O]. Gerontology 2006;52:223‐30. - PubMed
-
- Saltvedt I, Opdahl Mo ES, Fayers P, Kaasa S, Sletvold O. Reduced mortality in treating acutely sick, frail older patients in a geriatric evaluation and management unit. A prospective randomised trial. Journal of the American Geriatrics Society 2002;50:792‐8. - PubMed
-
- Saltvedt I, Spigset O, Ruths S, Fayers P, Kaasa S, Sletvold O. Patterns of drug prescription in a geriatric evaluation and management unit as compared with the general medical wards: a randomised study. European Journal of Clinical Pharmacology 2005;61:921‐8. - PubMed
-
- Satvedt I, Saltnes T, Opdahl Mo ES, Fayers P, Kaasa S, Sletvold O. Acute geriatric intervention increases the number of patients able to live at home. A prospective randomised study. Aging Clinical and Experimental Research 2004;16(4):300‐6. - PubMed
Shamian 1984 {published data only}
-
- Shamian J, Clarfield AM, Maclean J. A randomized trial of intra‐hospital relocation of geriatric patients in a tertiary‐care teaching hospital. Journal of the American Geriatrics Society 1984;32:794‐800. [MEDLINE: ] - PubMed
Somme 2010 {published and unpublished data}
-
- Somme D, Andrieux N, Guerot E, Lahjibi‐Paulet H, Lazarovici C, Gisselbrecht M, et al. Loss of autonomy among elderly patients after a stay in a medical intensive care unit (ICU): a randomised study of the benefit of transfer to a geriatric ward. Archives of Gerontology and Geriatrics 2010;50:e36‐e40. - PubMed
Thomas 1993 {published data only}
-
- Thomas DR, Brahan R, Haywood BP. Inpatient community‐based geriatric assessment reduces subsequent mortality. Journal of the American Geriatrics Society 1993;41:101‐4. - PubMed
Wald 2011 {published and unpublished data}
-
- Wald HL, Glasheen JJ, Guerrasio J, Youngwerth JM, Cumbler EU. Evaluation of a hospitalist‐run acute care for the elderly service. Journal of Hospital Medicine 2011;6(6):313‐21. - PubMed
White 1994 {published data only}
-
- White SJ, Powers JS, Knight JR, Harrell D, Varnell L, Vaughn C, et al. Effectiveness of an inpatient geriatric service in a university hospital. Journal of the Tennessee Medical Association 1994;87:425‐8. - PubMed
Winograd 1993 {published data only}
-
- Winograd CH, Gerety MB, Lai NA. A negative trial of inpatient geriatric consultation. Archives of Internal Medicine 1993;153:2017‐23. - PubMed
References to studies excluded from this review
Abizanda 2011 {published and unpublished data}
-
- Abizanda P, Leon M, Dominguez‐Martin L, Lozano‐Berrio V, Romero L, Luengo C, et al. Effects of a short‐term occupational therapy intervention in an acute geriatric unit. A randomized clinical trial. Maturitas 2011;69(3):273‐8. - PubMed
Borok 1994 {published data only}
-
- Borok GM, Reuben DB, Zendle LJ, Ershoff DH, Wolde‐Tsadik G. Rationale and design of a multi‐centre randomized trial of comprehensive geriatric assessment consultation for hospitalised patients in an RMO. Journal of the American Geriatrics Society 1994;42(5):536‐44. - PubMed
Boult 1994 {published data only}
-
- Boult C, Boult L, Murphy C, Ebbitt B, Luptak M. Controlled trial of outpatient geriatric evaluation and management. Journal of the American Geriatrics Society 1994;42(5):465‐70. - PubMed
Campion 1983 {published data only}
-
- Campion EW, Jette A, Berkman B. Interdisciplinary geriatric consultation service: a controlled trial. Journal of the American Geriatrics Society 1983;31(12):792‐6. - PubMed
Cole 1991 {published data only}
-
- Cole MG, Fenton FR, Engelsmann F, Mansouri I. Effectiveness of geriatric psychiatry consultation in an acute care hospital: a randomized clinical trial. Journal of the American Geriatrics Society 1991;39(12):1183‐8. - PubMed
Cunliffe 2004 {published data only}
-
- Cunliffe AL, Gladman JRF, Husbands SL, Miller P, Dewey ME, Harwood RH. Sooner and healthier: a randomised controlled trial and interview study of an early discharge rehabilitation service for older people. Age & Ageing 2004;33:246‐52. - PubMed
Epstein 1990 {published data only}
-
- Epstein AM, Hall JA, Fretwell M, Feldstein M, DeCiantis ML. Consultative geriatric assessment for ambulatory patients. JAMA 1990;263(4):538‐44. - PubMed
Fleming 2004 {published data only}
-
- Fleming SA, Blake H, Gladman JRF, Hart E, Lymberry M, Dewey ME, et al. A randomised controlled trial of a care home rehabilitation service to reduce long‐term institutionalisation for elderly people. Age & Ageing 33;4:384‐90. - PubMed
Garåsen 2007 {published data only}
Gayton 1987 {published data only}
-
- Gayton D, Wood‐Dauphinee S, Lorimer M, Tousignant P, Hanley J. Trial of a geriatric consultation team in an acute care hospital. Journal of the American Geriatrics Society 1987;35(8):726‐36. - PubMed
Germain 1995 {published data only}
-
- Germain M, Knoeffel F, Wieland D, Rubenstein LZ. A geriatric assessment and intervention team for hospital inpatients awaiting transfer to a geriatric unit: a randomized trial. Aging ‐ Clinical and Experimental Research 1995;7(1):55‐60. - PubMed
Gharacholou 2012 {published and unpublished data}
-
- Gharacholou SM, Sloane R, Cohen HJ, Schmader KE. Geriatric inpatient units in the care of hospitalized frail adults with a history of heart failure. International Journal of Gerontology 2012;6(2):112‐6.
Gill 2003 {published data only}
-
- Gill TM, Baker DI, Gottschalk M, Gahbauer EA, Charpentier PA, Regt PT, et al. A rehabilitation programme for physically frail community living older persons. Archives of Physical Medicine and Rehabilitation 2003;84:394‐404. - PubMed
-
- Gill TM, McGloin JM, Gahbauer EA, Shepard DM, Bianco LM. Two recruitment strategies for a clinical trial of physically frail community‐living older persons. Journal of the American Geriatrics Society 2001;49:1039‐45. - PubMed
Harari 2007 {published data only}
-
- Harari D, Martin FC, Buttery A, O'Neill S, Hopper A. The older persons' assessment and liaison team 'OPAL': evaluation of comprehensive geriatric assessment in acute medical inpatients. Age & Ageing 2007;36(6):670‐5. - PubMed
Hogan 1990 {published data only}
-
- Hogan DB. Impact of geriatric consultation services for elderly patients admitted to acute care hospitals. Canadian Journal on Aging 1990;9(1):35‐44.
-
- Hogan DB, Fox RA. A prospective controlled trial of a geriatric consultation team in an acute‐care hospital. Age & Ageing 1990;19:107‐13. - PubMed
Karppi 1995 {published data only}
-
- Karppi P. Effects of a geriatric inpatient unit on elderly home‐care patients: a controlled trial. Aging Clinical and Experimental Research 1995;7:207‐11. - PubMed
-
- Karppi P, Tilvis R. Effectiveness of a Finnish geriatric inpatient assessment. Two‐year follow‐up of a randomized clinical trial on community‐dwelling patients. Scandinavian Journal of Primary Health Care 1995;13(2):93‐8. - PubMed
Kehusmaa 2010 {published and unpublished data}
-
- Kehusmaa S, Autti‐Ramao I, Valaste M, Hinkka K, Rissanen P. Economic evaluation of a geriatric rehabilitation programme: a randomised controlled trial. Journal of Rehabilitation Medicine 2010;42(10):949‐55. - PubMed
Landi 1997 {published data only}
-
- Landi F, Zuccala G, Bernabei R, Cocchi A, Manigrasso L, Tafani A, et al. Physiotherapy and occupational therapy: a geriatric experience in the acute care hospital. American Journal of Physical Medicine and Rehabilitation 1997;76(1):38‐42. - PubMed
Ledesert 1994 {published data only}
-
- Ledesert B, Lombrail P, Yeni P, Carbon C, Brodin M. The impact of a comprehensive multi‐dimensional geriatric assessment programme on duration of stay in a French acute medical ward. Age & Ageing 1994;23:223‐7. - PubMed
Liem 1986 {published data only}
-
- Liem PH, Chernoff R, Carter WJ. Geriatric rehabilitation unit: a 3‐year outcome evaluation. Journal of Gerontology 1986;41(1):44‐50. - PubMed
Meissner 1989 {published data only}
-
- Meissner P, Andolsek K, Mears PA, Fletcher B. Maximising the functional status of geriatric patients in an acute community hospital setting. The Gerontologist 1989;29(4):524‐8. - PubMed
Miller 1996 {published data only}
-
- Miller DK, Lewis L, Nork MJ, Morley JE. Controlled trial of a geriatric case‐finding and liaison service in an emergency department. Journal of the American Geriatrics Society 1996;44(5):513‐20. - PubMed
Mudge 2006 {published data only}
-
- Mudge A, Laracy S, Richter K, Denaro C. Controlled trial of multidisciplinary care teams for acutely ill medical inpatients: enhanced multidisciplinary care. Internal Medicine Journal 2006;36:558‐63. - PubMed
Mudge 2012 {published and unpublished data}
-
- Mudge AM, Denaro CP, O'Rourke P. Improving hospital outcomes in patients admitted from residential aged care: results from a controlled trial. Age and Ageing 2012;41(5):670‐3. - PubMed
Nipp 2012 {published and unpublished data}
Retornaz 2007 {published data only}
-
- Retornaz F, Seux V, Sourial N, Braud AC, Monette J, Bergman H, et al. Comparison of health and functional status between older inpatients with and without cancer admitted to a Geriatric/Internal Medicine Unit. The Journals of Gerontology 2007;62A:917‐22. - PubMed
Reuben 1992 {published data only}
-
- Reuben DB, Wolde‐Tsadik G, Pardamean B, Hammond B, Borok GM, Rubenstein LZ, et al. The use of targeting criteria in hospitalized HMO patients: results from the demonstration phase of the Hospitalised Older Persons Evaluation (HOPE) study. Journal of the American Geriatrics Society 1992;40:482‐8. - PubMed
Rubin 1992 {published data only}
-
- Rubin CD, Sizemore MT, Loftis PA, Adams‐Huet B, Anderson RJ. The effect of geriatric evaluation and management on medicare reimbursement in a large public hospital: a randomized clinical trial. Journal of the American Geriatrics Society 1992;40:989‐95. - PubMed
-
- Rubin CD, Sizemore MT, Loftis PA, Loret de Mola N. Randomized controlled trial of outpatient geriatric evaluation and management in a large public hospital. Journal of the American Geriatrics Society 1993;41(10):1023‐8. - PubMed
Trentini 2001 {published data only}
-
- Trentini M, Semeraro S, Motta M. Effectiveness of geriatric evaluation and care. One‐year results of a multicenter randomized clinical trial. Aging ‐ Clinical and Experimental Research 2001;13(5):395‐405. - PubMed
Volicer 1994 {published data only}
-
- Volicer L, Collard A, Hurley A, Bishop C, Kern D, Karon S. Impact of special care unit for patients with advanced Alzheimer's disease on patient discomfort and costs. Journal of the American Geriatrics Society 1994;42:597‐603. - PubMed
Yoo 2013a {published and unpublished data}
-
- Yoo JW, Kim S, Seol H, Kim SJ, Yang JM Ryu WS, et al. Effects of an internal medicine floor interdisciplinary team on hospital and clinical outcomes of seniors with acute medical illness. Geriatrics and Gerontology International 2013;13(4):942‐8. - PubMed
Yoo 2013b {published and unpublished data}
-
- Yoo JW, Nakagawa S, Kim S. Delirium and transition to a nursing home of hospitalized older adults: a controlled trial of assessing the interdisciplinary team‐based geriatric care and care coordinated by non‐geriatrics specialist physicians. Geriatrics and Gerontology International 2013;13(2):342‐50. - PubMed
Yoo 2014 {published and unpublished data}
-
- Yoo JW, Seol H, Kim SJ, Yang JM, Ryu WS, Min TD, et al. Effects of hospitalist‐directed interdisciplinary medicine floor service on hospital outcomes for seniors with acute medical illness. Geriatrics and Gerontology International 2014;14(1):71‐7. - PubMed
Young 2005 {published data only}
-
- Green J, Young J, Forster A. Background to the post‐acute care trial of community hospital rehabilitation for older people. International Journal of Therapy and Rehabilitation 2006;13(2):66‐73.
-
- Small N, Green J, Spink J, Forster A, Lowson K, Young J. The patient experience of community hospital ‐ the process of care as a determinant of satisfaction. Journal of Evaluation in Clinical Practice 2007;13(1):95‐101. - PubMed
-
- Young J, Forster A, Green J, Bogle S. Post‐acute transfer of older people to intermediate care services: the sooner the better?. Age & Ageing 2007;36(5):589‐92. - PubMed
Additional references
Bachmann 2010
Bakker 2011
-
- Bakker FC, Robben SHM, Olde Rikkert MGM. Effects of hospital‐wide interventions to improve care for frail older inpatients: a systematic review. BMJ Quality and Safety 2011;doi:10.1136:/bmjqs.2010.047183. - PubMed
Barnett 2012
-
- Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross‐sectional study. Lancet 2012;380:37‐43. - PubMed
Baztan 2009
-
- Baztán JJ, Suárez‐García FM, López‐Arrieta J, Rodríguez‐Mañas L, Rodríguez‐Artalejo F. Effectiveness of acute geriatric units on functional decline, living at home, and case fatality among older patients admitted to hospital for acute medical disorders: meta‐analysis. BMJ 2009;338:b50. - PMC - PubMed
Baztan 2011
-
- Baztan JJ, Suarez‐Garcia FM, Lopez‐Arrieta J, Rodriguez‐Manaz L. Efficiency of acute geriatric units: a meta‐analysis of controlled studies. Revista Española de Geriatría y Gerontología 2011;46:186‐92. - PubMed
Clegg 2013
Cochran 1954
-
- Cochran WG. The combination of estimates from different experiments. Biometrics 1954;10:101‐29.
Conroy 2011
-
- Conroy SP, Stevens T, Parker SG, Gladman JRF. A systematic review of comprehensive geriatric assessment to improve outcomes for frail older people being rapidly discharged from acute hospital: 'interface geriatrics'. Age Ageing 2011;40:436‐43. - PubMed
Deeks 2001
-
- Deeks J, Altman D, Bradburn MJ. Statistical methods for examining heterogeneity and combining results from several studies in meta‐analysis. Egger M, Davey Smith G, Altman DG, editors. Systematic Reviews in Health Care. Meta‐analysis in Context. New York, New York: Wiley, 2001:285‐312.
DerSimonian 1986
-
- DerSimonian R, Laird N. Meta‐analysis in clinical trials. Controlled Clinical Trials 1986;7:177‐88. - PubMed
Edmans 2011
Ellis 2011
Ellis 2005
-
- Ellis G, Langhorne P. Comprehensive geriatric assessment for older hospital patients. British Medical Bulletin 2005;71:45‐59. - PubMed
EPOC 2017a
-
- Effective Practice, Organisation of Care (EPOC). Data collection form. EPOC resources for review authors, 2017. Available from epoc.cochrane.org/epoc‐resources‐review‐authors.
EPOC 2017b
-
- Effective Practice, Organisation of Care (EPOC). Suggested risk of bias criteria for EPOC reviews. EPOC resources for review authors, 2017. Available from epoc.cochrane.org/epoc‐specific‐resources‐review‐authors.
EPOC 2017c
-
- Effective Practice, Organisation of Care (EPOC). EPOC worksheets for preparing a 'Summary of findings' table using GRADE. EPOC resources for review authors, 2017. Available from epoc.cochrane.org/epoc‐specific‐resources‐review‐authors.
Extermann 2007
-
- Extermann M, Hurria A. Comprehensive geriatric assessment for older patients with cancer. Journal of Clinical Oncology 2007;25(14):1824‐31. - PubMed
Francis 2013
-
- Francis R. Report of the Mid Staffordshire NHS Foundation Trust Public Inquiry. London: The Stationary Office, 2013.
GRADEpro GDT 2015 [Computer program]
-
- McMaster University (developed by Evidence Prime). GRADEpro GDT. Version accessed prior to 10 August 2017. Hamilton (ON): McMaster University (developed by Evidence Prime), 2015.
Guyatt 2008
Handoll 2009
Harwood 2011
-
- Harwood RH, Goldberg SE, Whittamore KH, Russell C, Gladman JRF, Jones RG, et al. Medical Crises in Older People Study Group (MCOP). Evaluation of a medical and mental health unit compared with standard care for older people whose emergency admission to an acute general hospital is complicated by concurrent 'confusion': a controlled clinical trial. TEAM: Trial of an Elderly Acute care Medical and mental health unit. Trials 2011;12:123. - PMC - PubMed
Higgins 2003
Higgins 2011
-
- Higgins JP, Green S, editor(s). Cochrane Handbook of Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org. www.cochrane‐handbook.org: The Cochrane Collaboration.
Kaambwa 2013
-
- Kaambwa B, Billingham L, Bryan S. Mapping utility scores from the Barthel index. European Journal of Health Economics 2013;14:231‐41. - PubMed
Melis 2008
-
- Melis RJF, Adang E, Teerenstra S, Eijken MIJ, Wimo A, Achterberg T, et al. Multidimensional geriatric assessment: back to the future: cost‐effectiveness of a multidisciplinary intervention model for community‐dwelling frail older people. Journals of Gerontology, Series A. Biological Sciences and Medical Sciences 2008;63(3):275‐82. - PubMed
Morganti 2013
-
- Morganti KG, Bauhoff S, Blanchard JC, Abir M, Iyer N, Smith AC, et al. The evolving role of emergency departments in the United States, 2013. www.rand.org/content/dam/rand/pubs/research_reports/RR200/RR280/RAND_RR2... (accessed 20 May 2016). - PMC - PubMed
National Audit Office 2013
-
- National Audit Office (NAO). Report by the Comptroller and Auditor General. Emergency admissions to hospital: managing the demand. National Audit Office 30 October 2013.
NICE 2013
-
- NICE National Institute for Health and Care Excellence. Process and methods guides. Guide to the methods of technology appraisal, 2013. publications.nice.org.uk/pmg9 4 April 2013:1‐102.
Review Manager 2014 [Computer program]
-
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Royal College of Physicians 2012
-
- Royal College of Physicians. Hospitals on the Edge? The time for action. A report by the Royal College of Physicians 2012;www.rcplondon.ac.uk/guidelines‐policy/hospitals‐edge‐time‐action:1‐8.
Rubenstein 1991
-
- Rubenstein LZ, Stuck AE, Siu AL, Wieland D. Impact of geriatric evaluation and management programs on defined outcomes: overview of the evidence. Journal of the American Geriatrics Society. 1991; Vol. 39:8S‐16S. - PubMed
Rudd 1997
Shemilt 2011
-
- Shemilt I, Mugford M, Byford S, Drummond M, Eisenstein E, Knapp M, et al. Chapter 15: Incorporating economics evidence. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
STATA 13 [Computer program]
-
- StataCorp. Stata Statistical Software: Release 13.. College Station, TX: StataCorp LP, 2013.
Stuck 1993
-
- Stuck AE, Siu AL, Wieland D, Adams J, Rubenstein LZ. Comprehensive geriatric assessment: a meta‐analysis of controlled trials. Lancet 1993;342:1032‐6. - PubMed
SUTC 2013
Tanajewski 2015
-
- Tanajewski L, Franklin M, Ghountouras G, Berdunov V, Edmans J, Conroy S, et al. Cost‐effectiveness of a specialist geriatric medical intervention for frail older people discharged from acute medical units: economic evaluation in a two‐centre randomised controlled trial (AMIGOS). PLOS ONE 2015;10(5):doi:10.1371/journal.pone.0121340. - PMC - PubMed
The Lancet 2014
-
- Editorial. Global elderly care in crisis. The Lancet 2014;383:doi:10.1016/S0140‐6736(14)60463‐3.
Thompson 1999
-
- Thompson SG, Sharp SJ. Explaining heterogeneity in meta‐analysis: a comparison of methods. Statistics in Medicine 1999;18:2693‐708. - PubMed
Van Craen 2010
-
- Craen K, Braes T, Wellens N, Denhaerynck K, Flamaing J, Moons P, et al. The effectiveness of inpatient geriatric evaluation and management units: a systematic review and meta‐analysis. Journal of the American Geriatrics Society 2010;58:83‐92. - PubMed
van Exel 2004
-
- Exel NJ, Scholte op Reimer WJ, Koopmanschap MA. Assessment of post‐stroke quality of life in cost‐effectiveness studies: the usefulness of the Barthel index and the EuroQoL‐5D. Quality of Life Research 2004;13:427‐33. - PubMed
WHO 2016
-
- World Health Organization. World Health Statistics 2016: Monitoring Health for the SDGs, Sustainable Development Goals. Geneva, Switzerland: WHO Press, 2016.
References to other published versions of this review
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous