

Nebivolol Desensitizes Myofilaments of a Hypertrophic Cardiomyopathy Mouse Model
- PMID: 28824454
- PMCID: PMC5539082
- DOI: 10.3389/fphys.2017.00558
Nebivolol Desensitizes Myofilaments of a Hypertrophic Cardiomyopathy Mouse Model
Abstract
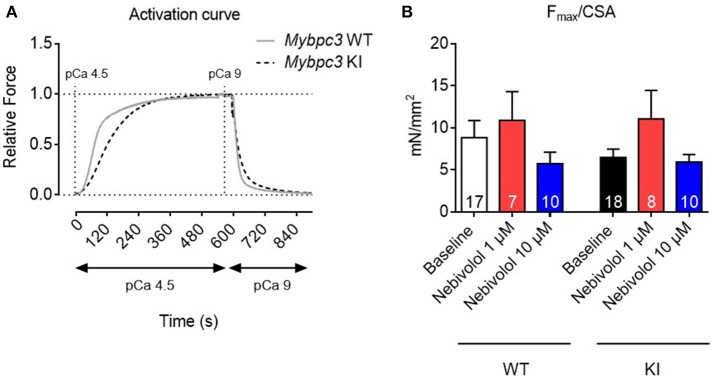
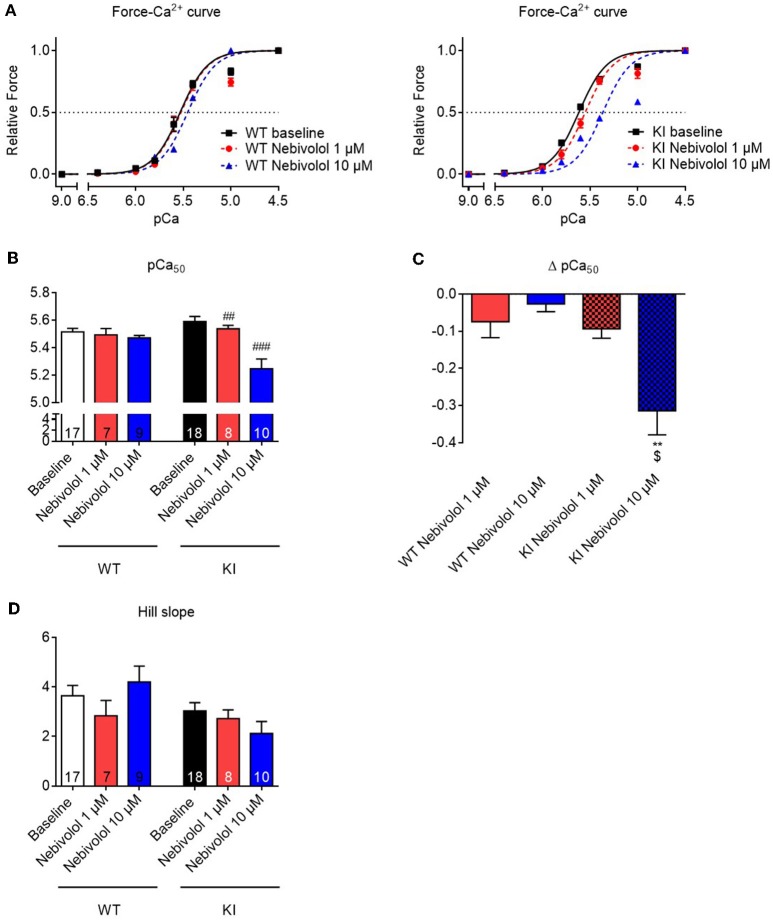
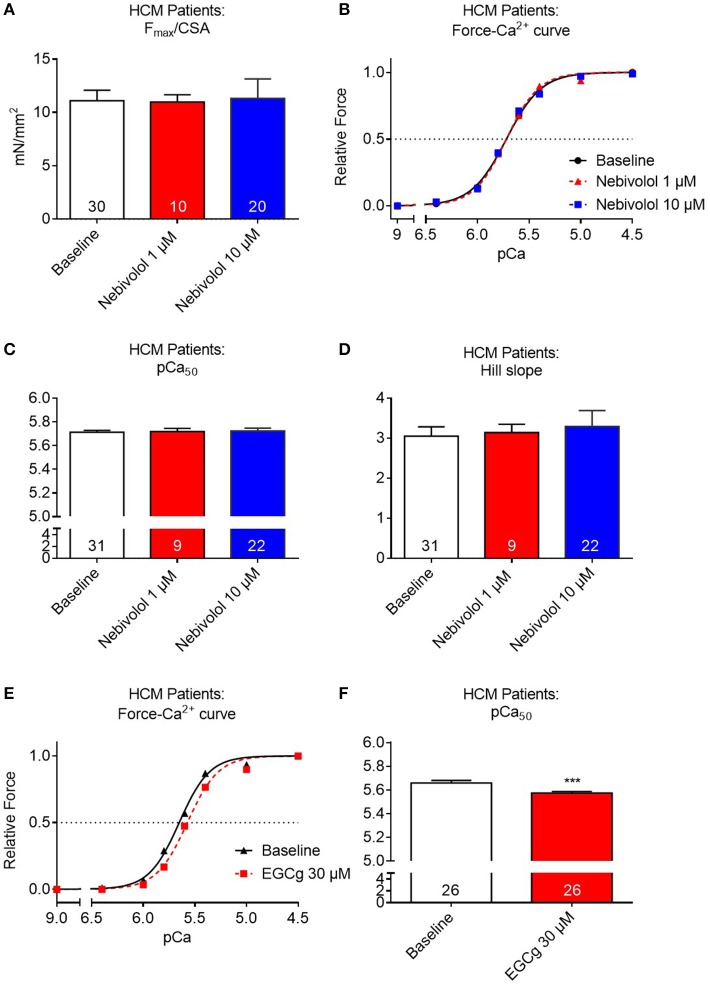
Background: Hypertrophic cardiomyopathy (HCM) patients often present with diastolic dysfunction and a normal to supranormal systolic function. To counteract this hypercontractility, guideline therapies advocate treatment with beta-adrenoceptor and Ca2+ channel blockers. One well established pathomechanism for the hypercontractile phenotype frequently observed in HCM patients and several HCM mouse models is an increased myofilament Ca2+ sensitivity. Nebivolol, a commonly used beta-adrenoceptor antagonist, has been reported to lower maximal force development and myofilament Ca2+ sensitivity in rabbit and human heart tissues. The aim of this study was to evaluate the effect of nebivolol in cardiac muscle strips of an established HCM Mybpc3 mouse model. Furthermore, we investigated actions of nebivolol and epigallocatechin-gallate, which has been shown to desensitize myofilaments for Ca2+ in mouse and human HCM models, in cardiac strips of HCM patients with a mutation in the most frequently mutated HCM gene MYBPC3. Methods and Results: Nebivolol effects were tested on contractile parameters and force-Ca2+ relationship of skinned ventricular muscle strips isolated from Mybpc3-targeted knock-in (KI), wild-type (WT) mice and cardiac strips of three HCM patients with MYBPC3 mutations. At baseline, KI strips showed no difference in maximal force development compared to WT mouse heart strips. Neither 1 nor 10 μM nebivolol had an effect on maximal force development in both genotypes. 10 μM nebivolol induced myofilament Ca2+ desensitization in WT strips and to a greater extent in KI strips. Neither 1 nor 10 μM nebivolol had an effect on Ca2+ sensitivity in cardiac muscle strips of three HCM patients with MYBPC3 mutations, whereas epigallocatechin-gallate induced a right shift in the force-Ca2+ curve. Conclusion: Nebivolol induced a myofilament Ca2+ desensitization in both WT and KI strips, which was more pronounced in KI muscle strips. In human cardiac muscle strips of three HCM patients nebivolol had no effect on myofilament Ca2+ sensitivity.
Keywords: Ca2+ sensitivity; Mybpc3; epigallocatechin-3-gallate; human; hypertrophic cardiomyopathy; mouse; myofilament; nebivolol.
Figures
Similar articles
-
Epigallocatechin-3-Gallate Accelerates Relaxation and Ca2+ Transient Decay and Desensitizes Myofilaments in Healthy and Mybpc3-Targeted Knock-in Cardiomyopathic Mice.Front Physiol. 2016 Dec 5;7:607. doi: 10.3389/fphys.2016.00607. eCollection 2016. Front Physiol. 2016. PMID: 27994558 Free PMC article.
-
Translational investigation of electrophysiology in hypertrophic cardiomyopathy.J Mol Cell Cardiol. 2021 Aug;157:77-89. doi: 10.1016/j.yjmcc.2021.04.009. Epub 2021 May 3. J Mol Cell Cardiol. 2021. PMID: 33957110 Free PMC article.
-
Diltiazem prevents stress-induced contractile deficits in cardiomyocytes, but does not reverse the cardiomyopathy phenotype in Mybpc3-knock-in mice.J Physiol. 2017 Jun 15;595(12):3987-3999. doi: 10.1113/JP273769. Epub 2017 Feb 7. J Physiol. 2017. PMID: 28090637 Free PMC article.
-
The Genetic and Molecular Bases for Hypertrophic Cardiomyopathy: The Role for Calcium Sensitization.J Cardiothorac Vasc Anesth. 2018 Feb;32(1):478-487. doi: 10.1053/j.jvca.2017.05.035. Epub 2017 May 19. J Cardiothorac Vasc Anesth. 2018. PMID: 29203298 Review.
-
Energetic drain driving hypertrophic cardiomyopathy.FEBS Lett. 2019 Jul;593(13):1616-1626. doi: 10.1002/1873-3468.13496. Epub 2019 Jul 4. FEBS Lett. 2019. PMID: 31209876 Review.
Cited by
-
Small Molecules acting on Myofilaments as Treatments for Heart and Skeletal Muscle Diseases.Int J Mol Sci. 2020 Dec 16;21(24):9599. doi: 10.3390/ijms21249599. Int J Mol Sci. 2020. PMID: 33339418 Free PMC article. Review.
-
Pushing the Limits of Medical Management in HCM: A Review of Current Pharmacological Therapy Options.Int J Mol Sci. 2021 Jul 5;22(13):7218. doi: 10.3390/ijms22137218. Int J Mol Sci. 2021. PMID: 34281272 Free PMC article. Review.
-
Disease modeling of a mutation in α-actinin 2 guides clinical therapy in hypertrophic cardiomyopathy.EMBO Mol Med. 2019 Dec;11(12):e11115. doi: 10.15252/emmm.201911115. Epub 2019 Nov 3. EMBO Mol Med. 2019. PMID: 31680489 Free PMC article.
-
Analysis of Contractile Function of Permeabilized Human Hypertrophic Cardiomyopathy Multicellular Heart Tissue.Front Physiol. 2019 Mar 28;10:239. doi: 10.3389/fphys.2019.00239. eCollection 2019. Front Physiol. 2019. PMID: 30984009 Free PMC article.
-
Phosphomimetic cardiac myosin-binding protein C partially rescues a cardiomyopathy phenotype in murine engineered heart tissue.Sci Rep. 2019 Dec 3;9(1):18152. doi: 10.1038/s41598-019-54665-2. Sci Rep. 2019. PMID: 31796859 Free PMC article.
References
-
- Alves M. L., Dias F. A., Gaffin R. D., Simon J. N., Montminy E. M., Biesiadecki B. J., et al. . (2014). Desensitization of myofilaments to Ca2+ as a therapeutic target for hypertrophic cardiomyopathy with mutations in thin filament proteins. Circ Cardiovasc Genet 7, 132–143. 10.1161/CIRCGENETICS.113.000324 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous