

Strategic Targeting of Multiple BMP Receptors Prevents Trauma-Induced Heterotopic Ossification
- PMID: 28716575
- PMCID: PMC5542633
- DOI: 10.1016/j.ymthe.2017.01.008
Strategic Targeting of Multiple BMP Receptors Prevents Trauma-Induced Heterotopic Ossification
Abstract
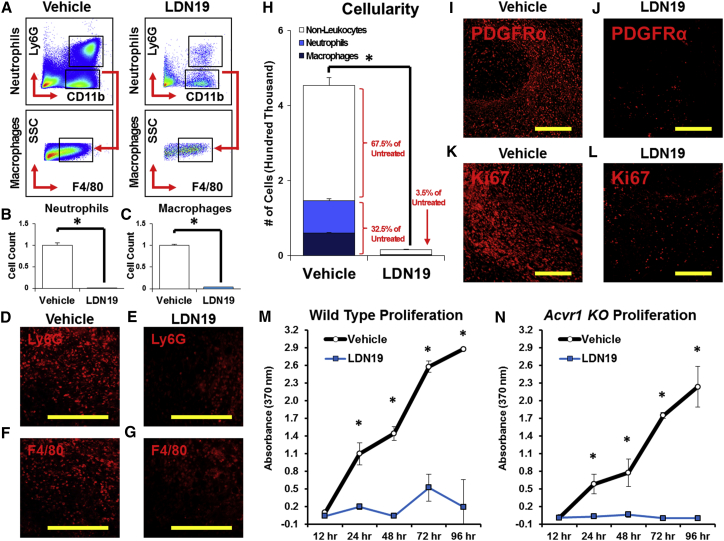
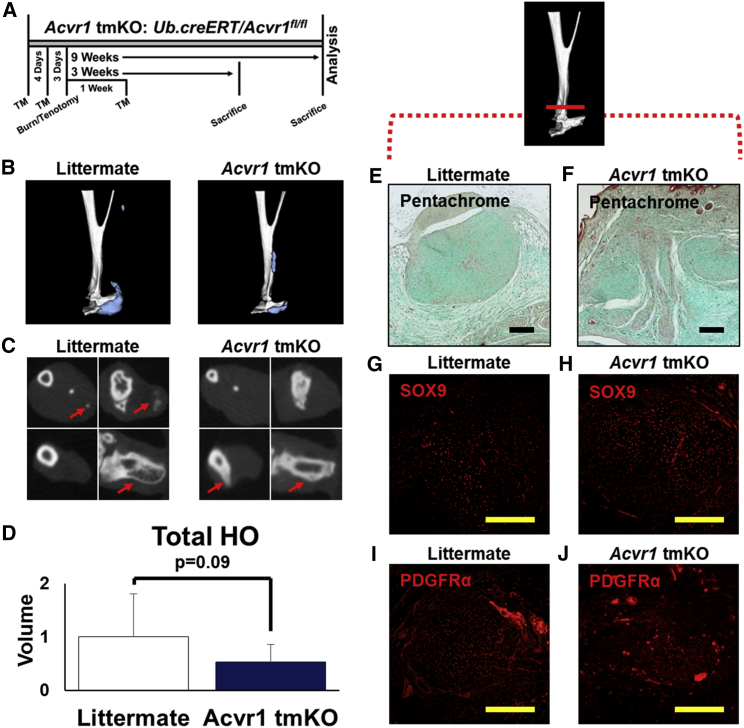
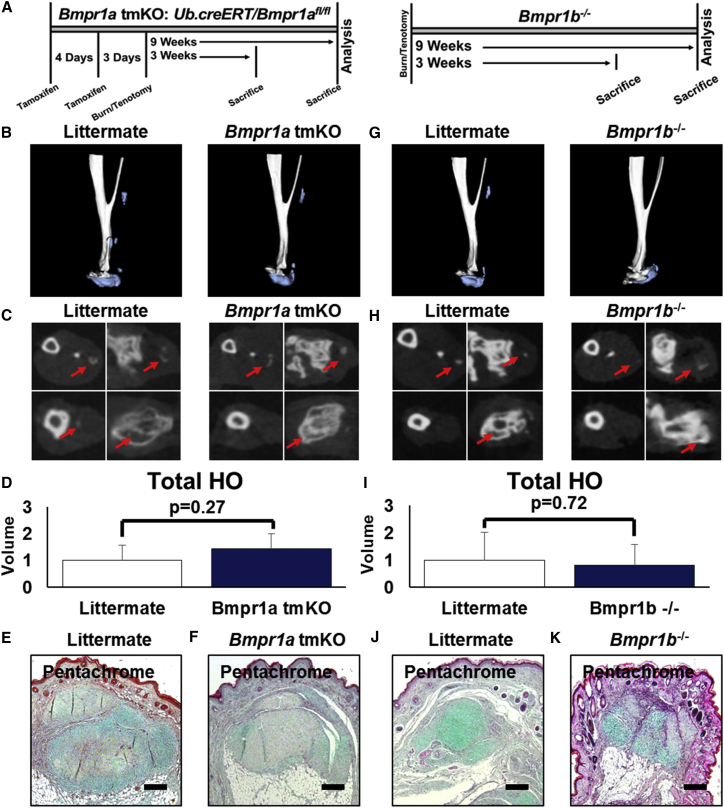
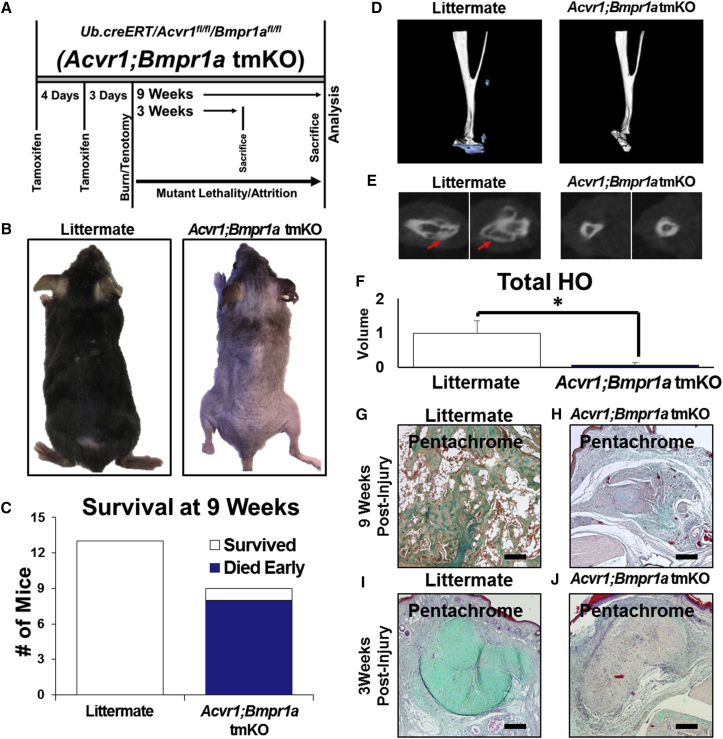
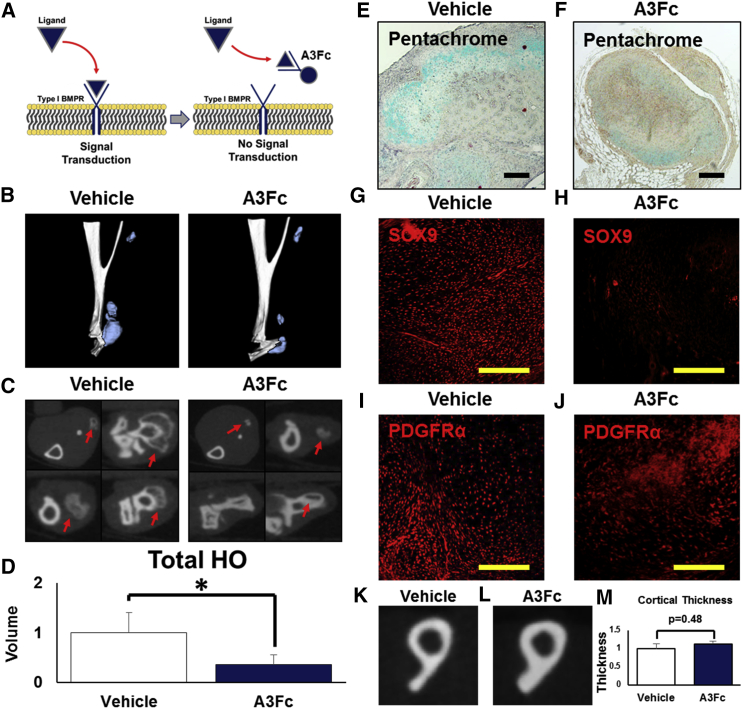
Trauma-induced heterotopic ossification (tHO) is a condition of pathologic wound healing, defined by the progressive formation of ectopic bone in soft tissue following severe burns or trauma. Because previous studies have shown that genetic variants of HO, such as fibrodysplasia ossificans progressiva (FOP), are caused by hyperactivating mutations of the type I bone morphogenetic protein receptor (T1-BMPR) ACVR1/ALK2, studies evaluating therapies for HO have been directed primarily toward drugs for this specific receptor. However, patients with tHO do not carry known T1-BMPR mutations. Here we show that, although BMP signaling is required for tHO, no single T1-BMPR (ACVR1/ALK2, BMPR1a/ALK3, or BMPR1b/ALK6) alone is necessary for this disease, suggesting that these receptors have functional redundancy in the setting of tHO. By utilizing two different classes of BMP signaling inhibitors, we developed a translational approach to treatment, integrating treatment choice with existing diagnostic options. Our treatment paradigm balances either immediate therapy with reduced risk for adverse effects (Alk3-Fc) or delayed therapy with improved patient selection but greater risk for adverse effects (LDN-212854).
Keywords: BMP receptors; BMP signaling; stem cells.
Copyright © 2017 The American Society of Gene and Cell Therapy. Published by Elsevier Inc. All rights reserved.
Figures

Similar articles
-
BMP Ligand Trap ALK3-Fc Attenuates Osteogenesis and Heterotopic Ossification in Blast-Related Lower Extremity Trauma.Stem Cells Dev. 2021 Jan 15;30(2):91-105. doi: 10.1089/scd.2020.0162. Epub 2020 Dec 24. Stem Cells Dev. 2021. PMID: 33256557 Free PMC article.
-
Activin A does not drive post-traumatic heterotopic ossification.Bone. 2020 Sep;138:115473. doi: 10.1016/j.bone.2020.115473. Epub 2020 Jun 15. Bone. 2020. PMID: 32553795
-
Alk2/ACVR1 and Alk3/BMPR1A Provide Essential Function for Bone Morphogenetic Protein-Induced Retinal Angiogenesis.Arterioscler Thromb Vasc Biol. 2017 Apr;37(4):657-663. doi: 10.1161/ATVBAHA.116.308422. Epub 2017 Feb 23. Arterioscler Thromb Vasc Biol. 2017. PMID: 28232325 Free PMC article.
-
Structural basis for the potent and selective binding of LDN-212854 to the BMP receptor kinase ALK2.Bone. 2018 Apr;109:251-258. doi: 10.1016/j.bone.2017.09.004. Epub 2017 Sep 12. Bone. 2018. PMID: 28918311 Free PMC article. Review.
-
Hints on transcriptional control of essential players in heterotopic ossification of Fibrodysplasia Ossificans Progressiva.Bone. 2018 Apr;109:187-191. doi: 10.1016/j.bone.2017.10.028. Epub 2017 Oct 31. Bone. 2018. PMID: 29100956 Review.
Cited by
-
Macrophage TGF-β signaling is critical for wound healing with heterotopic ossification after trauma.JCI Insight. 2022 Oct 24;7(20):e144925. doi: 10.1172/jci.insight.144925. JCI Insight. 2022. PMID: 36099022 Free PMC article.
-
Functional Testing of Bone Morphogenetic Protein (BMP) Pathway Variants Identified on Whole-Exome Sequencing in a Patient with Delayed-Onset Fibrodysplasia Ossificans Progressiva (FOP) Using ACVR1R206H -Specific Human Cellular and Zebrafish Models.J Bone Miner Res. 2022 Nov;37(11):2058-2076. doi: 10.1002/jbmr.4711. Epub 2022 Nov 15. J Bone Miner Res. 2022. PMID: 36153796 Free PMC article.
-
Role of the NF-kB signalling pathway in heterotopic ossification: biological and therapeutic significance.Cell Commun Signal. 2024 Mar 4;22(1):159. doi: 10.1186/s12964-024-01533-w. Cell Commun Signal. 2024. PMID: 38439078 Free PMC article. Review.
-
Intersections of Fibrodysplasia Ossificans Progressiva and Traumatic Heterotopic Ossification.Biomolecules. 2024 Mar 14;14(3):349. doi: 10.3390/biom14030349. Biomolecules. 2024. PMID: 38540768 Free PMC article. Review.
-
Developmentally inspired programming of adult human mesenchymal stromal cells toward stable chondrogenesis.Proc Natl Acad Sci U S A. 2018 May 1;115(18):4625-4630. doi: 10.1073/pnas.1720658115. Epub 2018 Apr 16. Proc Natl Acad Sci U S A. 2018. PMID: 29666250 Free PMC article.
References
-
- Forsberg J.A., Potter B.K. Heterotopic ossification in wartime wounds. J. Surg. Orthop. Adv. 2010;19:54–61. - PubMed
-
- Forsberg J.A., Pepek J.M., Wagner S., Wilson K., Flint J., Andersen R.C., Tadaki D., Gage F.A., Stojadinovic A., Elster E.A. Heterotopic ossification in high-energy wartime extremity injuries: prevalence and risk factors. J. Bone Joint Surg. Am. 2009;91:1084–1091. - PubMed
-
- Potter B.K., Forsberg J.A., Davis T.A., Evans K.N., Hawksworth J.S., Tadaki D., Brown T.S., Crane N.J., Burns T.C., O’Brien F.P., Elster E.A. Heterotopic ossification following combat-related trauma. J. Bone Joint Surg. Am. 2010;92(Suppl 2):74–89. - PubMed
-
- Kung T.A., Jebson P.J., Cederna P.S. An individualized approach to severe elbow burn contractures. Plast. Reconstr. Surg. 2012;129:663e–673e. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
