

High dose IVIG successfully reduces high rhGAA IgG antibody titers in a CRIM-negative infantile Pompe disease patient
- PMID: 28648664
- PMCID: PMC5612830
- DOI: 10.1016/j.ymgme.2017.05.006
High dose IVIG successfully reduces high rhGAA IgG antibody titers in a CRIM-negative infantile Pompe disease patient
Abstract
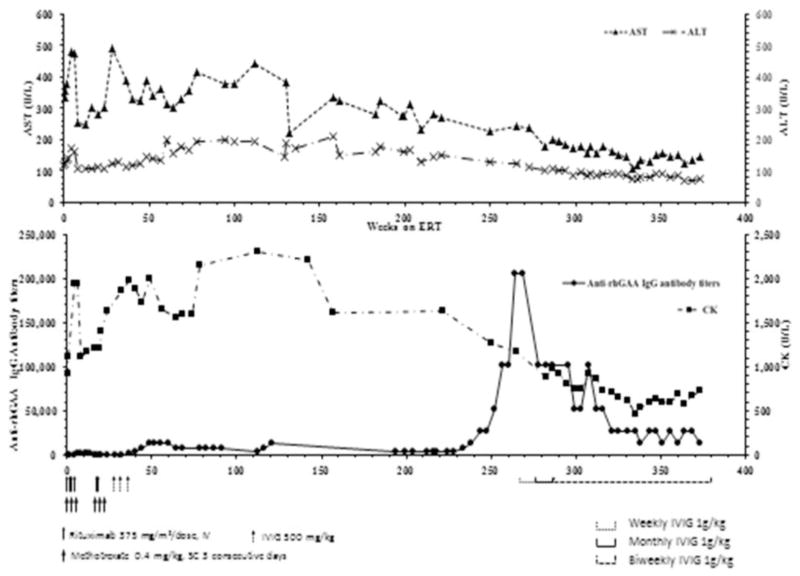
Alglucosidase alfa (rhGAA) has altered the course of an otherwise fatal outcome in classic infantile Pompe disease (IPD), which presents with cardiomyopathy and severe musculoskeletal involvement. However, the response to therapy is determined by several factors including the development of high and sustained antibody titers (HSAT) to rhGAA. Cross-reactive immunologic material (CRIM) negative patients are at the highest risk for development of HSAT. Immune tolerance induction (ITI) with methotrexate, rituximab, and intravenous immunoglobulin (IVIG) has been largely successful in preventing the immune response and in achieving tolerance when done in conjunction with enzyme replacement therapy (ERT) initiation. Reducing antibody titers in cases with an entrenched immune response remains a challenge in the field despite the use of multiple immunomodulatory agents. Success has been shown with addition of bortezomib to the ITI regimen, yet the prolonged course and potential risks with the use of such agents' demands caution. We present here a 7-year-old CRIM-negative IPD patient who was not successfully tolerized by an ITI regimen with rituximab, methotrexate, and IVIG due to intolerability to the regimen and recurrent infections. She went on to develop HSAT, with significant clinical decline, loss of all motor abilities, and a fragile medical state, which made it challenging to institute the bortezomib based regimen to reduce HSAT. She had severe developmental delay, respiratory failure with invasive ventilation and tracheostomy, persistent hypotonia, ptosis of eyelids, diffuse severe osteopenia, contractures, and was completely G-tube fed. As a rescue mechanism, we treated her with high dose and high frequency IVIG in an attempt to reduce rhGAA IgG antibody titers (antibody titers; titers). Her titers saw a steady decline on weekly IVIG doses at 1g/kg for 20weeks. Subsequently when the IVIG regimen was altered to 1g/kg every month, rising titers were detected and therefore the regimen was changed to a biweekly regimen. High dose IVIG resulted in an eightfold decrease in antibody titers. Clinically, she showed improvement with partial recovery of previously lost motor abilities, especially hand movements and better head and neck control than before. The regimen was safely tolerated with no hospitalizations. The effectiveness of IVIG as a single agent, in this case with multiple comorbidities and fragile clinical status, was lifesaving and may represent an effective, perhaps lifesaving rescue approach to reduce antibody titers.
Keywords: Anti-rhGAA IgG antibodies; High dose IVIG; Immunogenicity; Immunomodulation; Pompe disease.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Optimizing treatment outcomes: immune tolerance induction in Pompe disease patients undergoing enzyme replacement therapy.Front Immunol. 2024 Apr 23;15:1336599. doi: 10.3389/fimmu.2024.1336599. eCollection 2024. Front Immunol. 2024. PMID: 38715621 Free PMC article. Clinical Trial.
-
Immunological challenges and approaches to immunomodulation in Pompe disease: a literature review.Ann Transl Med. 2019 Jul;7(13):285. doi: 10.21037/atm.2019.05.27. Ann Transl Med. 2019. PMID: 31392197 Free PMC article. Review.
-
An updated management approach of Pompe disease patients with high-sustained anti-rhGAA IgG antibody titers: experience with bortezomib-based immunomodulation.Front Immunol. 2024 Mar 8;15:1360369. doi: 10.3389/fimmu.2024.1360369. eCollection 2024. Front Immunol. 2024. PMID: 38524130 Free PMC article.
-
Benefits of Prophylactic Short-Course Immune Tolerance Induction in Patients With Infantile Pompe Disease: Demonstration of Long-Term Safety and Efficacy in an Expanded Cohort.Front Immunol. 2020 Aug 6;11:1727. doi: 10.3389/fimmu.2020.01727. eCollection 2020. Front Immunol. 2020. PMID: 32849613 Free PMC article.
-
Are Anti-rhGAA Antibodies a Determinant of Treatment Outcome in Adults with Late-Onset Pompe Disease? A Systematic Review.Biomolecules. 2023 Sep 19;13(9):1414. doi: 10.3390/biom13091414. Biomolecules. 2023. PMID: 37759814 Free PMC article. Review.
Cited by
-
Optimizing treatment outcomes: immune tolerance induction in Pompe disease patients undergoing enzyme replacement therapy.Front Immunol. 2024 Apr 23;15:1336599. doi: 10.3389/fimmu.2024.1336599. eCollection 2024. Front Immunol. 2024. PMID: 38715621 Free PMC article. Clinical Trial.
-
Immunological challenges and approaches to immunomodulation in Pompe disease: a literature review.Ann Transl Med. 2019 Jul;7(13):285. doi: 10.21037/atm.2019.05.27. Ann Transl Med. 2019. PMID: 31392197 Free PMC article. Review.
-
Advances in Immune Tolerance Induction in Enzyme Replacement Therapy.Paediatr Drugs. 2024 May;26(3):287-308. doi: 10.1007/s40272-024-00627-9. Epub 2024 Apr 25. Paediatr Drugs. 2024. PMID: 38664313 Free PMC article. Review.
-
Severe CNS involvement in a subset of long-term treated children with infantile-onset Pompe disease.Mol Genet Metab. 2024 Feb;141(2):108119. doi: 10.1016/j.ymgme.2023.108119. Epub 2023 Dec 22. Mol Genet Metab. 2024. PMID: 38184429 Free PMC article.
-
Immune responses to alglucosidase in infantile Pompe disease: recommendations from an Italian pediatric expert panel.Ital J Pediatr. 2022 Mar 5;48(1):41. doi: 10.1186/s13052-022-01219-4. Ital J Pediatr. 2022. PMID: 35248118 Free PMC article. Review.
References
-
- Kishnani PS, Hwu WL, Mandel H, Nicolino M, Yong F, Corzo D. A retrospective, multinational, multicenter study on the natural history of infantile-onset Pompe disease. J Pediatr. 2006;148:671–676.e672. - PubMed
-
- van den Hout HMP, Hop W, van Diggelen OP, Smeitink JAM, Smit GPA, Poll-The BTT, Bakker HD, Loonen MCB, de Klerk JBC, Reuser AJJ, van der Ploeg AT. The natural course of infantile Pompe’s disease: 20 original cases compared with 133 cases from the literature. Pediatrics. 2003;112:332–340. - PubMed
-
- Chien YH, Lee NC, Huang HJ, Thurberg BL, Tsai FJ, Hwu WL. Later-onset Pompe disease: early detection and early treatment initiation enabled by newborn screening. J Pediatr. 2011;158:1023–1027.e1021. - PubMed
-
- Kishnani PS, Beckemeyer AA, Mendelsohn NJ. The new era of Pompe disease: advances in the detection, understanding of the phenotypic spectrum, pathophysiology, and management. Am J Med Genet C: Semin Med Genet. 2012;160C:1–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
