

Mendelian randomization in cardiometabolic disease: challenges in evaluating causality
- PMID: 28569269
- PMCID: PMC5600813
- DOI: 10.1038/nrcardio.2017.78
Mendelian randomization in cardiometabolic disease: challenges in evaluating causality
Abstract
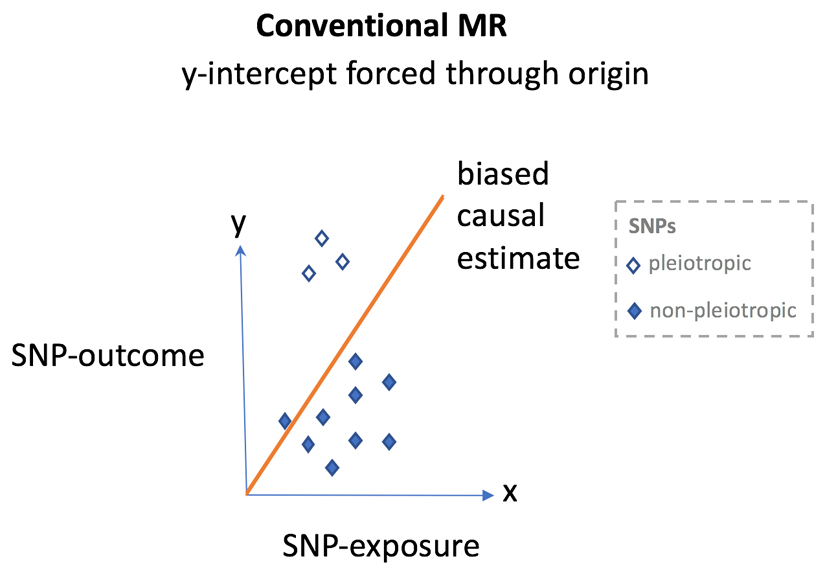
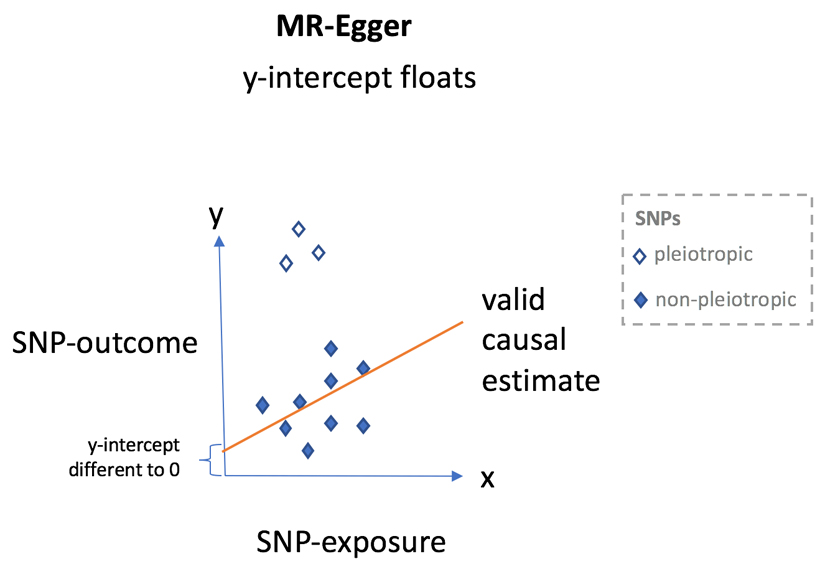
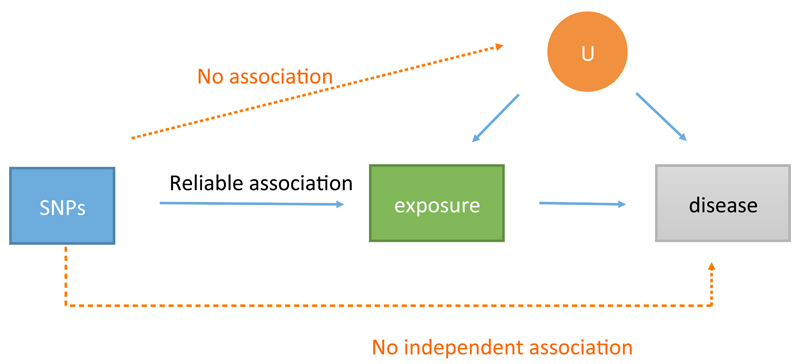
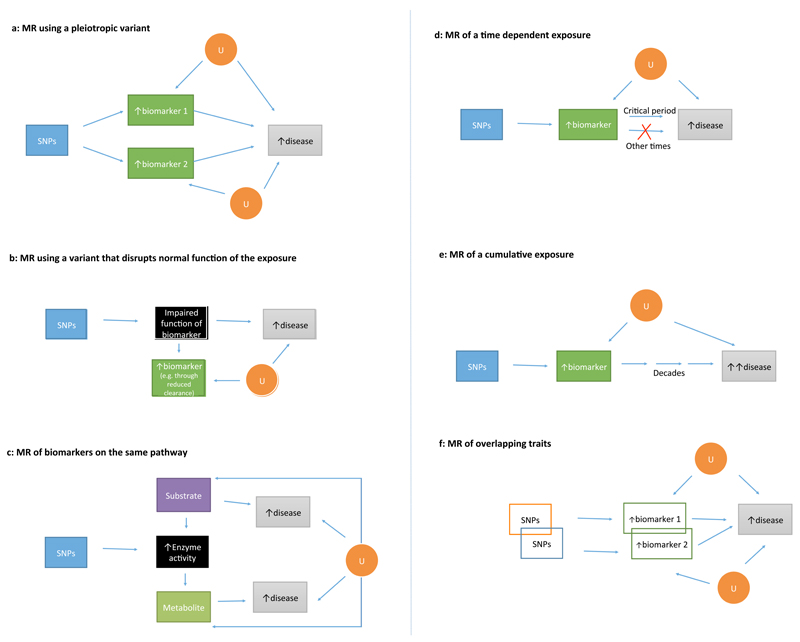
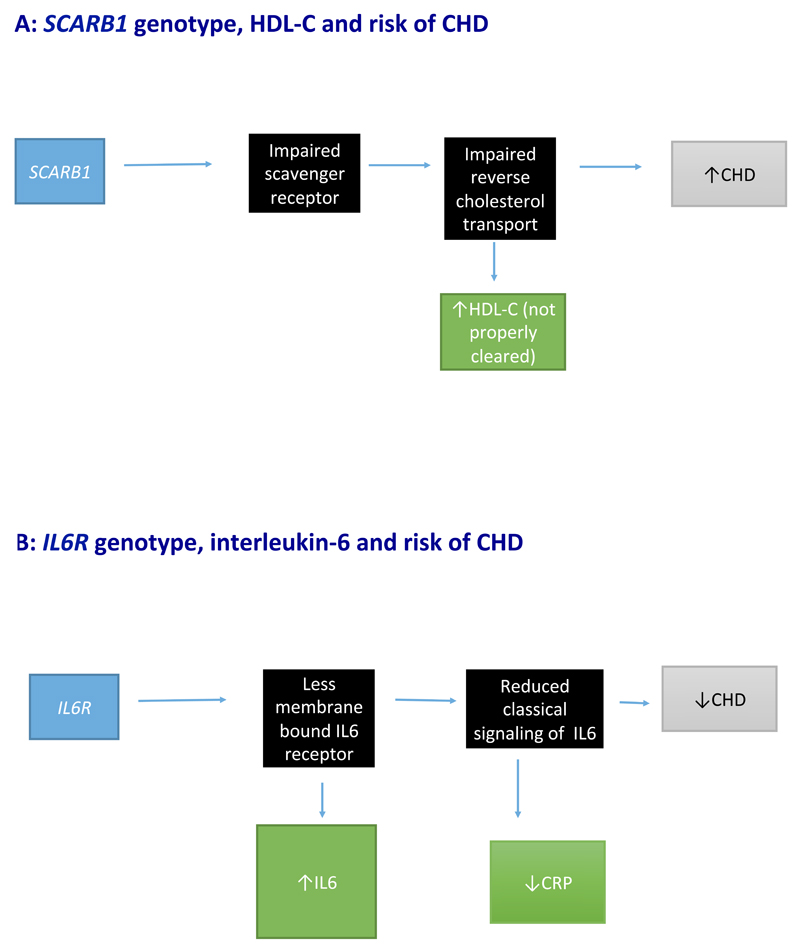
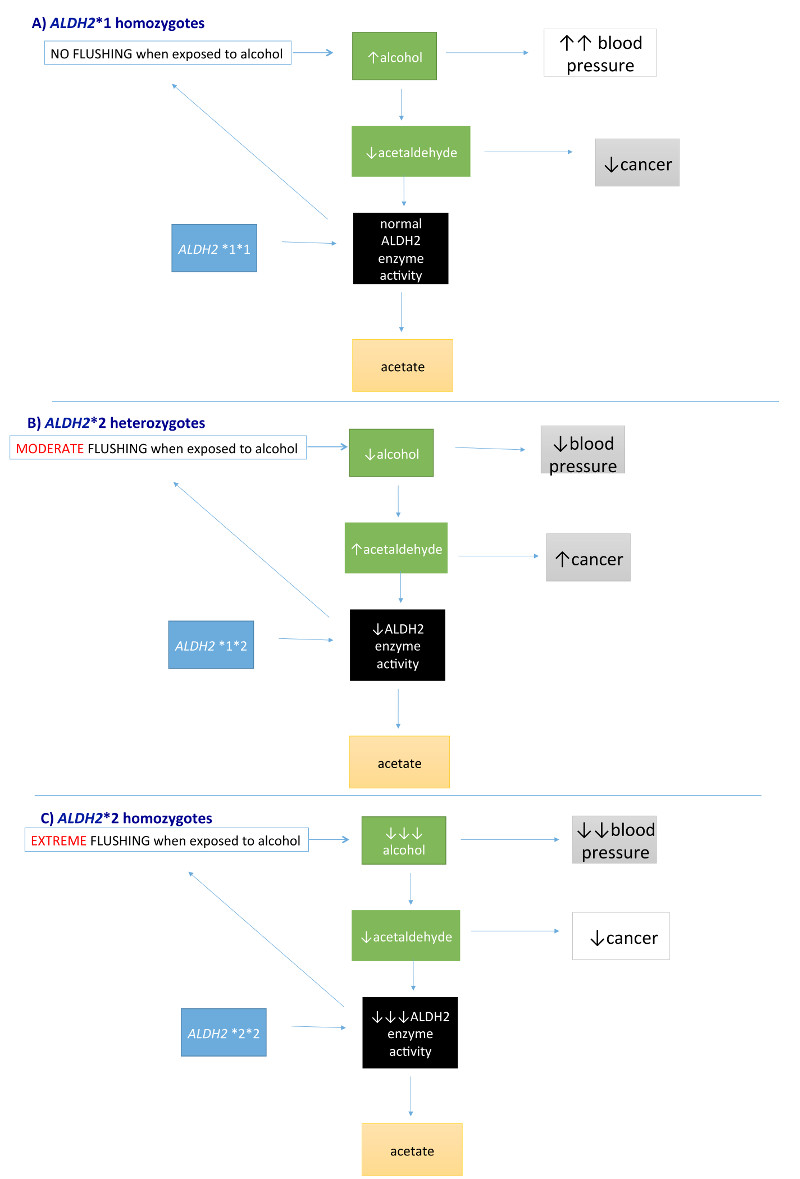
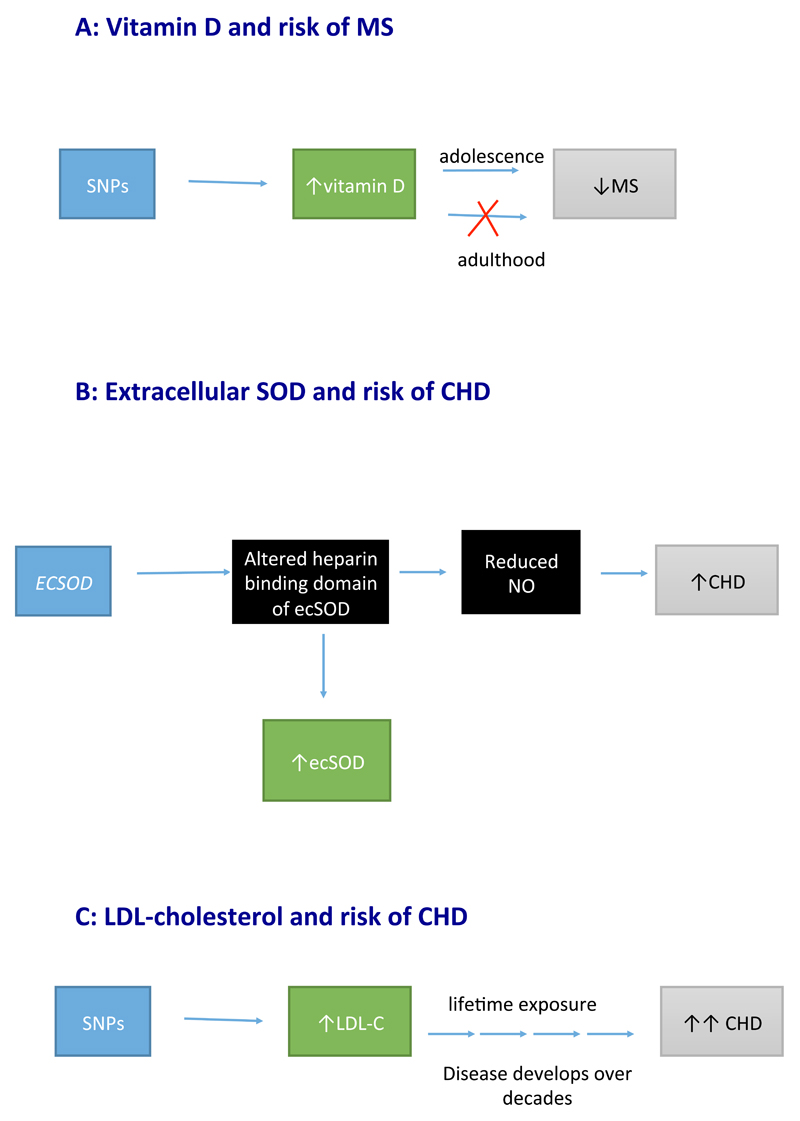
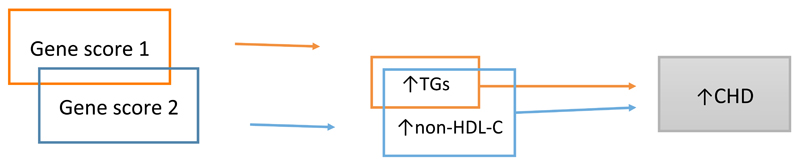
Mendelian randomization (MR) is a burgeoning field that involves the use of genetic variants to assess causal relationships between exposures and outcomes. MR studies can be straightforward; for example, genetic variants within or near the encoding locus that is associated with protein concentrations can help to assess their causal role in disease. However, a more complex relationship between the genetic variants and an exposure can make findings from MR more difficult to interpret. In this Review, we describe some of these challenges in interpreting MR analyses, including those from studies using genetic variants to assess causality of multiple traits (such as branched-chain amino acids and risk of diabetes mellitus); studies describing pleiotropic variants (for example, C-reactive protein and its contribution to coronary heart disease); and those investigating variants that disrupt normal function of an exposure (for example, HDL cholesterol or IL-6 and coronary heart disease). Furthermore, MR studies on variants that encode enzymes responsible for the metabolism of an exposure (such as alcohol) are discussed, in addition to those assessing the effects of variants on time-dependent exposures (extracellular superoxide dismutase), cumulative exposures (LDL cholesterol), and overlapping exposures (triglycerides and non-HDL cholesterol). We elaborate on the molecular features of each relationship, and provide explanations for the likely causal associations. In doing so, we hope to contribute towards more reliable evaluations of MR findings.
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Multivariable Mendelian randomization: the use of pleiotropic genetic variants to estimate causal effects.Am J Epidemiol. 2015 Feb 15;181(4):251-60. doi: 10.1093/aje/kwu283. Epub 2015 Jan 27. Am J Epidemiol. 2015. PMID: 25632051 Free PMC article.
-
Exploring the causal pathway from omega-6 levels to coronary heart disease: A network Mendelian randomization study.Nutr Metab Cardiovasc Dis. 2020 Feb 10;30(2):233-240. doi: 10.1016/j.numecd.2019.09.013. Epub 2019 Sep 16. Nutr Metab Cardiovasc Dis. 2020. PMID: 31648883
-
Mendelian randomization to assess causal effects of blood lipids on coronary heart disease: lessons from the past and applications to the future.Curr Opin Endocrinol Diabetes Obes. 2016 Apr;23(2):124-30. doi: 10.1097/MED.0000000000000230. Curr Opin Endocrinol Diabetes Obes. 2016. PMID: 26910273 Free PMC article. Review.
-
Mendelian randomization identifies blood metabolites previously linked to midlife cognition as causal candidates in Alzheimer's disease.Proc Natl Acad Sci U S A. 2021 Apr 20;118(16):e2009808118. doi: 10.1073/pnas.2009808118. Proc Natl Acad Sci U S A. 2021. PMID: 33879569 Free PMC article.
-
Mendelian randomization studies in coronary artery disease.Eur Heart J. 2014 Aug 1;35(29):1917-24. doi: 10.1093/eurheartj/ehu208. Epub 2014 Jun 10. Eur Heart J. 2014. PMID: 24917639 Review.
Cited by
-
Causal relationship between Women's reproductive traits and postpartum depression: a multivariate mendelian randomization analysis.Front Genet. 2024 Oct 11;15:1434762. doi: 10.3389/fgene.2024.1434762. eCollection 2024. Front Genet. 2024. PMID: 39464794 Free PMC article.
-
Relationship between alcohol consumption and dementia with Mendelian randomization approaches among older adults in the United States.medRxiv [Preprint]. 2023 Dec 22:2023.12.22.23300298. doi: 10.1101/2023.12.22.23300298. medRxiv. 2023. Update in: Alzheimers Dement (Amst). 2024 Jun 20;16(2):e12598. doi: 10.1002/dad2.12598 PMID: 38196582 Free PMC article. Updated. Preprint.
-
Integrating genomics with biomarkers and therapeutic targets to invigorate cardiovascular drug development.Nat Rev Cardiol. 2021 Jun;18(6):435-453. doi: 10.1038/s41569-020-00493-1. Epub 2021 Mar 11. Nat Rev Cardiol. 2021. PMID: 33707768 Review.
-
Insulin resistance and systemic metabolic changes in oral glucose tolerance test in 5340 individuals: an interventional study.BMC Med. 2019 Nov 29;17(1):217. doi: 10.1186/s12916-019-1440-4. BMC Med. 2019. PMID: 31779625 Free PMC article.
-
Genetic determinants of beverage consumption: Implications for nutrition and health.Adv Food Nutr Res. 2019;89:1-52. doi: 10.1016/bs.afnr.2019.03.001. Epub 2019 Apr 19. Adv Food Nutr Res. 2019. PMID: 31351524 Free PMC article. Review.
References
-
- Fewell Z, Davey Smith G, Sterne JA. The impact of residual and unmeasured confounding in epidemiologic studies: a simulation study. Am J Epidemiol. 2007;166:646–655. - PubMed
-
- Harrison RK. Phase II and phase III failures: 2013–2015. Nat Rev Drug Discov. 2016;15:817–818. - PubMed
-
- Fordyce CB, et al. Cardiovascular drug development: is it dead or just hibernating? J Am Coll Cardiol. 2015;65:1567–1582. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
