

Treatment of lung disease in alpha-1 antitrypsin deficiency: a systematic review
- PMID: 28496314
- PMCID: PMC5422329
- DOI: 10.2147/COPD.S130440
Treatment of lung disease in alpha-1 antitrypsin deficiency: a systematic review
Abstract
Background: Alpha-1 antitrypsin deficiency (AATD) is a rare genetic condition predisposing individuals to chronic obstructive pulmonary disease (COPD). The treatment is generally extrapolated from COPD unrelated to AATD; however, most COPD trials exclude AATD patients; thus, this study sought to systematically review AATD-specific literature to assist evidence-based patient management.
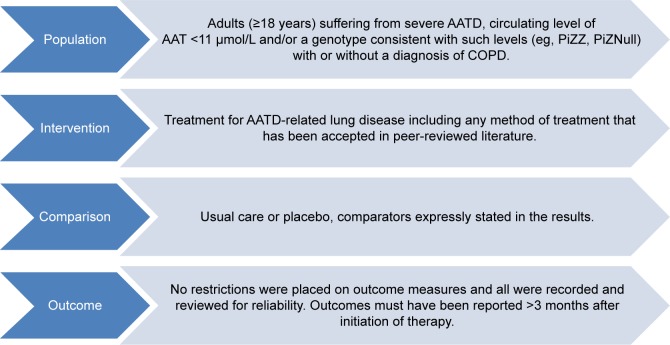
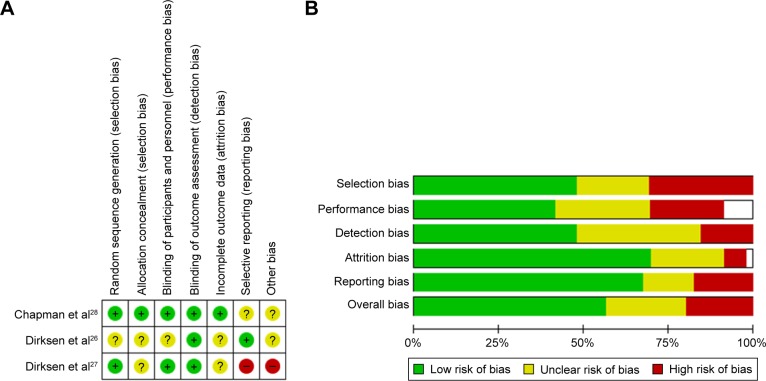
Methods: Standard review methodology was used with meta-analysis and narrative synthesis (PROSPERO-CRD42015019354). Eligible studies were those of any treatment used in severe AATD. Randomized controlled trials (RCTs) were the primary focus; however, case series and uncontrolled studies were eligible. All studies had ≥10 participants receiving treatment or usual care, with baseline and follow-up data (>3 months). Risk of bias was assessed appropriately according to study methodology.
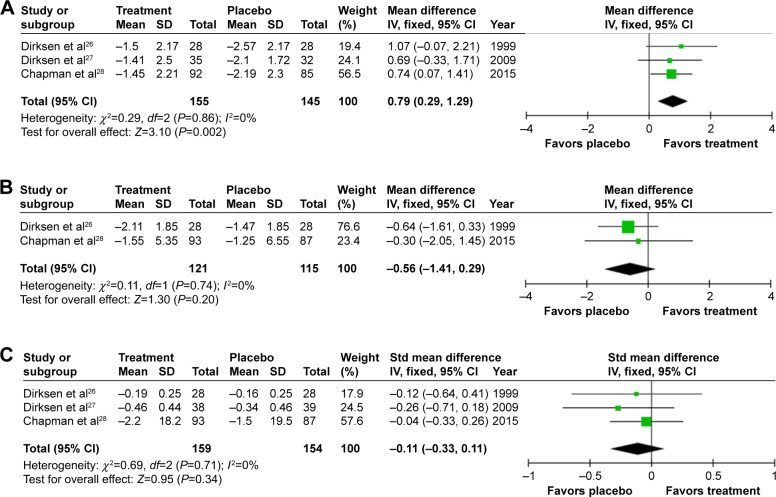
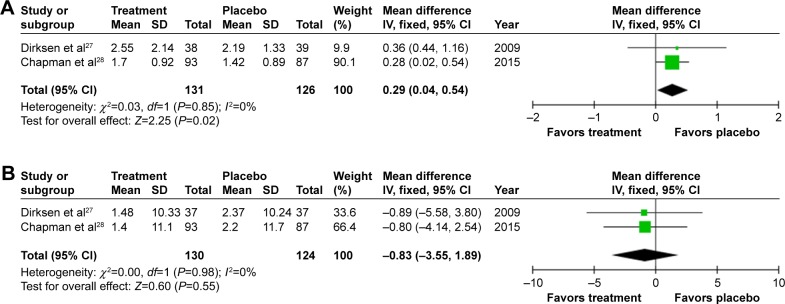
Results: In all, 7,296 studies were retrieved from searches; 52 trials with 5,632 participants met the inclusion criteria, of which 26 studies involved alpha-1 antitrypsin augmentation and 17 concerned surgical treatments (largely transplantation). Studies were grouped into four management themes: COPD medical, COPD surgical, AATD specific, and other treatments. Computed tomography (CT) density, forced expiratory volume in 1 s, diffusing capacity of the lungs for carbon monoxide, health status, and exacerbation rates were frequently used as outcomes. Meta-analyses were only possible for RCTs of intravenous augmentation, which slowed progression of emphysema measured by CT density change, 0.79 g/L/year versus placebo (P=0.002), and associated with a small increase in exacerbations 0.29/year (P=0.02). Mortality following lung transplant was comparable between AATD- and non-AATD-related COPD. Surgical reduction of lung volume demonstrated inferior outcomes compared with non-AATD-related emphysema.
Conclusion: Intravenous augmentation remains the only disease-specific therapy in AATD and there is evidence that this slows decline in emphysema determined by CT density. There is paucity of data around other treatments in AATD. Treatments for usual COPD may not be as efficacious in AATD, and further studies may be required for this disease group.
Keywords: alpha-1 antitrypsin deficiency; emphysema; transplantation; treatment.
Conflict of interest statement
Disclosure Mr Edgar reports grants from HEE and NIHR, during the conduct of the study. This article presents independent research funded by the NIHR. The views expressed are those of the authors and not necessarily those of the NHS, NIHR, HEE, or the Department of Health. Dr Patel, Mrs Bayliss, and Dr Crossley have nothing to disclose. Dr Sapey reports grants from NIHR, during the conduct of the study, and grants from Medical Research Council, Alpha-1 Foundation, and British Lung Foundation, outside the submitted work. Dr Turner reports grants from Grifols Biotherapeutics, Alpha-1 Foundation, outside the submitted work, and The Birmingham AATD Registry has received past funds from CSL Behring for work in AATD, although this was not held by any of the authors. The authors report no other conflicts of interest in this work.
Figures

Similar articles
-
Indications for active case searches and intravenous alpha-1 antitrypsin treatment for patients with alpha-1 antitrypsin deficiency chronic pulmonary obstructive disease: an update.Arch Bronconeumol. 2015 Apr;51(4):185-92. doi: 10.1016/j.arbres.2014.05.008. Epub 2014 Jul 12. Arch Bronconeumol. 2015. PMID: 25027067 English, Spanish.
-
Long-term clinical outcomes following treatment with alpha 1-proteinase inhibitor for COPD associated with alpha-1 antitrypsin deficiency: a look at the evidence.Respir Res. 2017 May 30;18(1):105. doi: 10.1186/s12931-017-0574-1. Respir Res. 2017. PMID: 28558837 Free PMC article. Review.
-
Diagnosis and treatment of lung disease associated with alpha one-antitrypsin deficiency: A position statement from the Thoracic Society of Australia and New Zealand.Respirology. 2020 Mar;25(3):321-335. doi: 10.1111/resp.13774. Epub 2020 Feb 6. Respirology. 2020. PMID: 32030868 Free PMC article. Review.
-
Matrix metalloproteinase-9 predicts pulmonary status declines in α1-antitrypsin deficiency.Respir Res. 2011 Mar 23;12(1):35. doi: 10.1186/1465-9921-12-35. Respir Res. 2011. PMID: 21429222 Free PMC article.
-
Nine controversial questions about augmentation therapy for alpha-1 antitrypsin deficiency: a viewpoint.Eur Respir Rev. 2023 Dec 6;32(170):230170. doi: 10.1183/16000617.0170-2023. Print 2023 Dec 31. Eur Respir Rev. 2023. PMID: 38056890 Free PMC article.
Cited by
-
Alpha-1 Antitrypsin Deficiency and Accelerated Aging: A New Model for an Old Disease?Drugs Aging. 2019 Sep;36(9):823-840. doi: 10.1007/s40266-019-00684-7. Drugs Aging. 2019. PMID: 31179525 Review.
-
Protein Misfolding and Aggregation: The Relatedness between Parkinson's Disease and Hepatic Endoplasmic Reticulum Storage Disorders.Int J Mol Sci. 2021 Nov 18;22(22):12467. doi: 10.3390/ijms222212467. Int J Mol Sci. 2021. PMID: 34830348 Free PMC article. Review.
-
Focus on Early COPD: Definition and Early Lung Development.Int J Chron Obstruct Pulmon Dis. 2021 Nov 25;16:3217-3228. doi: 10.2147/COPD.S338359. eCollection 2021. Int J Chron Obstruct Pulmon Dis. 2021. PMID: 34858022 Free PMC article. Review.
-
Predicting Lung Function Using Biomarkers in Alpha-1 Antitrypsin Deficiency.Biomedicines. 2023 Jul 15;11(7):2001. doi: 10.3390/biomedicines11072001. Biomedicines. 2023. PMID: 37509640 Free PMC article.
-
Can Common Lead Apron in Testes Region Cause Radiation Dose Reduction during Chest CT Scan? A Patient Study.J Biomed Phys Eng. 2021 Aug 1;11(4):497-504. doi: 10.31661/jbpe.v0i0.2104-1307. eCollection 2021 Aug. J Biomed Phys Eng. 2021. PMID: 34458197 Free PMC article.
References
-
- Eriksson S. Pulmonary emphysema and alpha1-antitrypsin deficiency. Acta Med Scandinavica. 1964;175:197–205. - PubMed
-
- Stockley RA, Turner AM. Alpha-1-Antitrypsin deficiency: clinical variability, assessment, and treatment. Trends Mol Med. 2014;20(2):105–115. - PubMed
-
- Laurell CB, Eriksson S. The serum α1-antitrypsin in families with hypo-α1-antitrypsinemia. Clin Chim Acta. 1965;11(5):395–398. - PubMed
-
- Laurell C-B, Eriksson S. The electrophoretic alpha1-globulin pattern of serum in alpha1-antitrypsin deficiency. 1963. COPD. 2013;10(Suppl 1):3–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
