

Metabolic Flexibility in Health and Disease
- PMID: 28467922
- PMCID: PMC5513193
- DOI: 10.1016/j.cmet.2017.04.015
Metabolic Flexibility in Health and Disease
Abstract
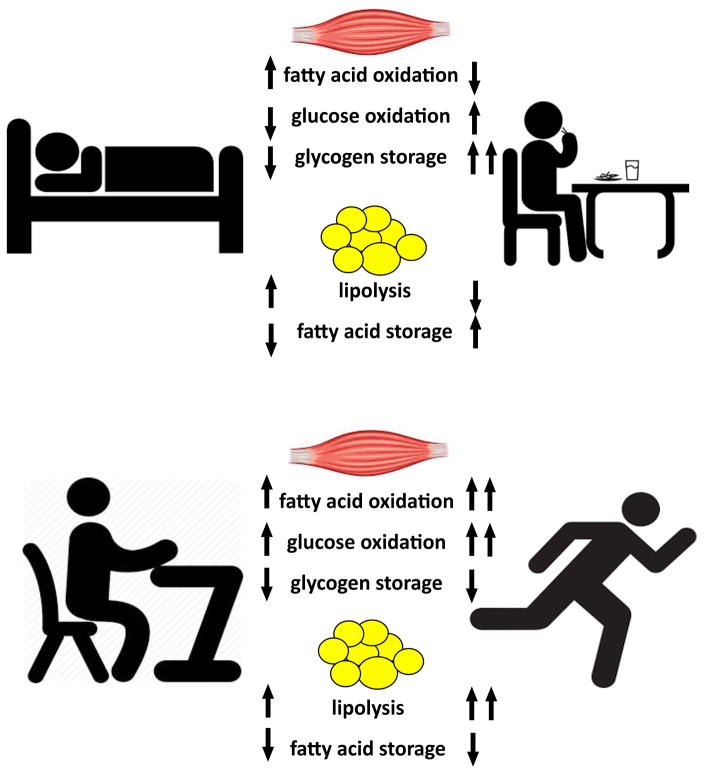
Metabolic flexibility is the ability to respond or adapt to conditional changes in metabolic demand. This broad concept has been propagated to explain insulin resistance and mechanisms governing fuel selection between glucose and fatty acids, highlighting the metabolic inflexibility of obesity and type 2 diabetes. In parallel, contemporary exercise physiology research has helped to identify potential mechanisms underlying altered fuel metabolism in obesity and diabetes. Advances in "omics" technologies have further stimulated additional basic and clinical-translational research to further interrogate mechanisms for improved metabolic flexibility in skeletal muscle and adipose tissue with the goal of preventing and treating metabolic disease.
Keywords: adipose tissue; exercise; insulin resistance; metabolic flexibility; obesity; skeletal muscle; type 2 diabetes.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Metabolic flexibility and obesity in children and youth.Obes Rev. 2011 May;12(5):e44-53. doi: 10.1111/j.1467-789X.2010.00812.x. Epub 2010 Oct 26. Obes Rev. 2011. PMID: 20977601 Review.
-
Skeletal muscle triglycerides: an aspect of regional adiposity and insulin resistance.Ann N Y Acad Sci. 2002 Jun;967:135-45. Ann N Y Acad Sci. 2002. PMID: 12079843 Review.
-
Mechanistic model of fuel selection in the muscle.J Theor Biol. 2006 Sep 7;242(1):151-63. doi: 10.1016/j.jtbi.2006.02.009. Epub 2006 Mar 30. J Theor Biol. 2006. PMID: 16574156
-
Metabolic flexibility in the development of insulin resistance and type 2 diabetes: effects of lifestyle.Obes Rev. 2009 Mar;10(2):178-93. doi: 10.1111/j.1467-789X.2008.00544.x. Epub 2009 Jan 15. Obes Rev. 2009. PMID: 19207879 Review.
-
Exercise as a tool to mitigate metabolic disease.Am J Physiol Cell Physiol. 2024 Sep 1;327(3):C587-C598. doi: 10.1152/ajpcell.00144.2024. Epub 2024 Jul 9. Am J Physiol Cell Physiol. 2024. PMID: 38981607 Free PMC article. Review.
Cited by
-
Regulation of the one carbon folate cycle as a shared metabolic signature of longevity.Nat Commun. 2021 Jun 9;12(1):3486. doi: 10.1038/s41467-021-23856-9. Nat Commun. 2021. PMID: 34108489 Free PMC article.
-
Maternal metabolic health drives mesenchymal stem cell metabolism and infant fat mass at birth.JCI Insight. 2021 Jul 8;6(13):e146606. doi: 10.1172/jci.insight.146606. JCI Insight. 2021. PMID: 34061777 Free PMC article.
-
The Na/K-ATPase α1/Src interaction regulates metabolic reserve and Western diet intolerance.Acta Physiol (Oxf). 2021 Jul;232(3):e13652. doi: 10.1111/apha.13652. Epub 2021 Apr 4. Acta Physiol (Oxf). 2021. PMID: 33752256 Free PMC article.
-
Task-Oriented Circuit Training as an Alternative to Ergometer-Type Aerobic Exercise Training after Stroke.J Clin Med. 2021 May 30;10(11):2423. doi: 10.3390/jcm10112423. J Clin Med. 2021. PMID: 34070731 Free PMC article.
-
Six HIT Sessions Improve Cardiorespiratory Fitness and Metabolic Flexibility in Insulin Resistant and Insulin Sensitive Adolescents with Obesity.Int J Environ Res Public Health. 2022 Aug 25;19(17):10568. doi: 10.3390/ijerph191710568. Int J Environ Res Public Health. 2022. PMID: 36078293 Free PMC article.
References
-
- Aas V, Bakke SS, Feng YZ, Kase ET, Jensen J, Bajpeyi S, Thoresen GH, Rustan AC. Are cultured human myotubes far from home? Cell Tissue Res. 2013;354:671–682. - PubMed
-
- Amati F, Dube JJ, Alvarez-Carnero E, Edreira MM, Chomentowski P, Coen PM, Switzer GE, Bickel PE, Stefanovic-Racic M, Toledo FG, et al. Skeletal muscle triglycerides, diacylglycerols, and ceramides in insulin resistance: another paradox in endurance-trained athletes? Diabetes. 2011;60:2588–2597. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
