

Private sector opportunities and threats to achieving malaria elimination in the Greater Mekong Subregion: results from malaria outlet surveys in Cambodia, the Lao PDR, Myanmar, and Thailand
- PMID: 28464945
- PMCID: PMC5414126
- DOI: 10.1186/s12936-017-1800-5
Private sector opportunities and threats to achieving malaria elimination in the Greater Mekong Subregion: results from malaria outlet surveys in Cambodia, the Lao PDR, Myanmar, and Thailand
Abstract
Background: The aim of this paper is to review multi-country evidence of private sector adherence to national regulations, guidelines, and quality-assurance standards for malaria case management and to document current coverage of private sector engagement and support through ACTwatch outlet surveys implemented in 2015 and 2016.
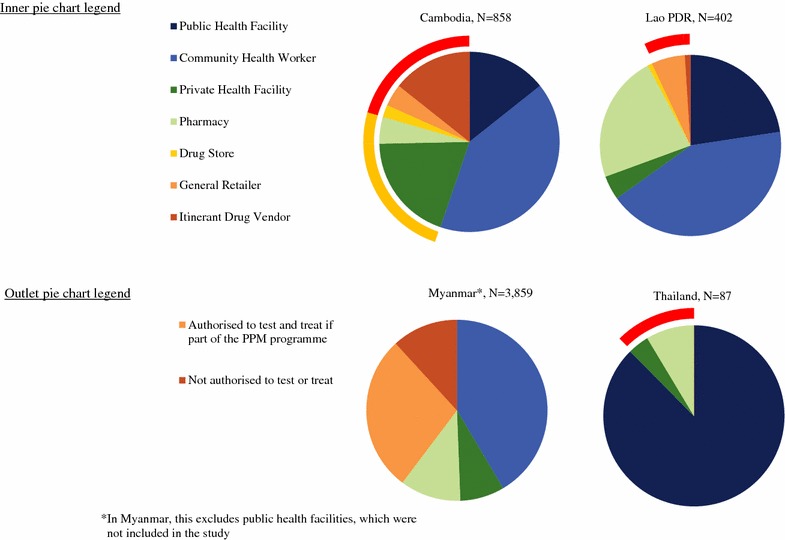
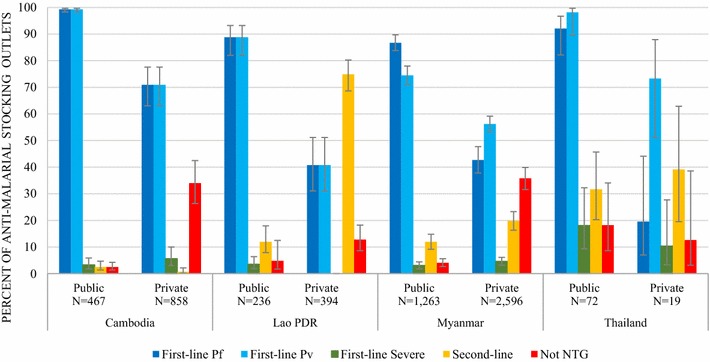
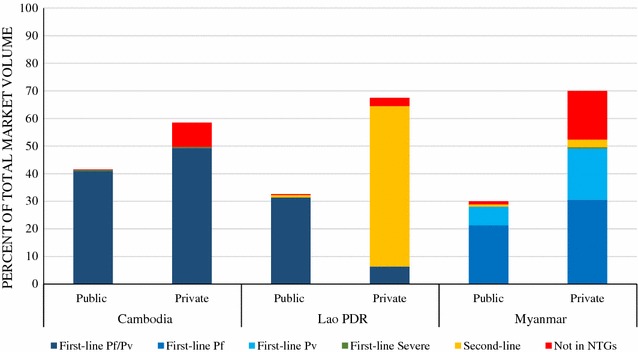
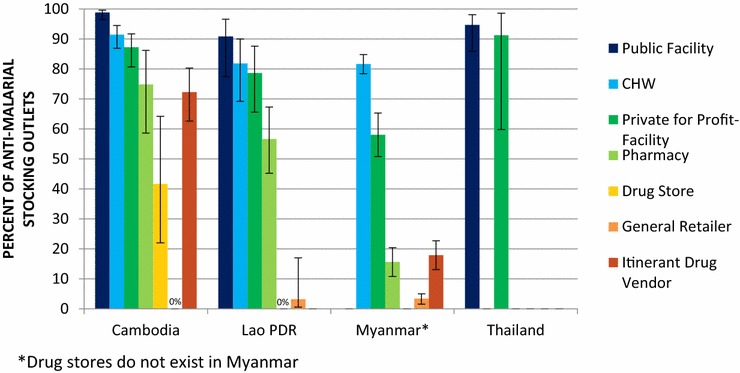
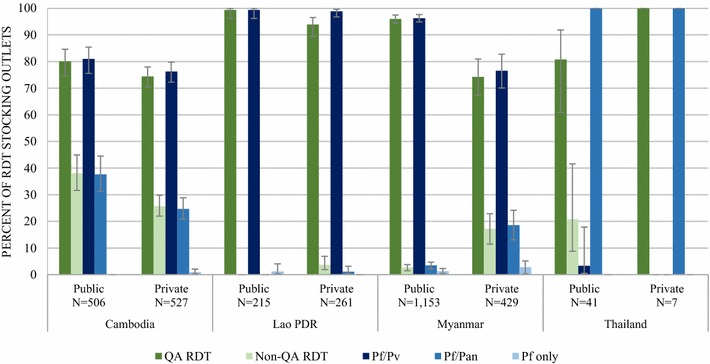
Results: Over 76,168 outlets were screened, and approximately 6500 interviews were conducted (Cambodia, N = 1303; the Lao People's Democratic Republic (PDR), N = 724; Myanmar, N = 4395; and Thailand, N = 74). There was diversity in the types of private sector outlets providing malaria treatment across countries, and the extent to which they were authorized to test and treat for malaria differed. Among outlets stocking at least one anti-malarial, public sector availability of the first-line treatment for uncomplicated Plasmodium falciparum or Plasmodium vivax malaria was >75%. In the anti-malarial stocking private sector, first-line treatment availability was variable (Cambodia, 70.9%; the Lao PDR, 40.8%; Myanmar P. falciparum = 42.7%, P. vivax = 19.6%; Thailand P. falciparum = 19.6%, P. vivax = 73.3%), as was availability of second-line treatment (the Lao PDR, 74.9%; Thailand, 39.1%; Myanmar, 19.8%; and Cambodia, 0.7%). Treatment not in the National Treatment Guidelines (NTGs) was most common in Myanmar (35.8%) and Cambodia (34.0%), and was typically stocked by the informal sector. The majority of anti-malarials distributed in Cambodia and Myanmar were first-line P. falciparum or P. vivax treatments (90.3% and 77.1%, respectively), however, 8.8% of the market share in Cambodia was treatment not in the NTGs (namely chloroquine) and 17.6% in Myanmar (namely oral artemisinin monotherapy). In the Lao PDR, approximately 9 in 10 anti-malarials distributed in the private sector were second-line treatments-typically locally manufactured chloroquine. In Cambodia, 90% of anti-malarials were distributed through outlets that had confirmatory testing available. Over half of all anti-malarial distribution was by outlets that did not have confirmatory testing available in the Lao PDR (54%) and Myanmar (59%). Availability of quality-assured rapid diagnostic tests (RDT) amongst the RDT-stocking public sector ranged from 99.3% in the Lao PDR to 80.1% in Cambodia. In Cambodia, the Lao PDR, and Myanmar, less than 50% of the private sector reportedly received engagement (access to subsidized commodities, supervision, training or caseload reporting), which was most common among private health facilities and pharmacies.
Conclusions: Findings from this multi-country study suggest that Cambodia, the Lao PDR, Myanmar, and Thailand are generally in alignment with national regulations, treatment guidelines, and quality-assurance standards. However, important gaps persist in the private sector which pose a threat to national malaria control and elimination goals. Several options are discussed to help align the private sector anti-malarial market with national elimination strategies.
Keywords: Anti-malarial; Availability; First-line; Greater Mekong Subregion (GMS); Market share; Private sector; RDT; Second-line.
Figures

Similar articles
-
The malaria testing and treatment landscape in the southern Lao People's Democratic Republic (PDR).Malar J. 2017 Apr 25;16(1):169. doi: 10.1186/s12936-017-1769-0. Malar J. 2017. PMID: 28438155 Free PMC article.
-
Anti-malarial landscape in Myanmar: results from a nationally representative survey among community health workers and the private sector outlets in 2015/2016.Malar J. 2017 Apr 25;16(1):129. doi: 10.1186/s12936-017-1761-8. Malar J. 2017. PMID: 28438197 Free PMC article.
-
Evidence on anti-malarial and diagnostic markets in Cambodia to guide malaria elimination strategies and policies.Malar J. 2017 Apr 25;16(1):171. doi: 10.1186/s12936-017-1807-y. Malar J. 2017. PMID: 28438204 Free PMC article.
-
Current status of human liver fluke infections in the Greater Mekong Subregion.Acta Trop. 2021 Dec;224:106133. doi: 10.1016/j.actatropica.2021.106133. Epub 2021 Sep 10. Acta Trop. 2021. PMID: 34509453 Review.
-
Malaria in the Greater Mekong Subregion: heterogeneity and complexity.Acta Trop. 2012 Mar;121(3):227-39. doi: 10.1016/j.actatropica.2011.02.016. Epub 2011 Mar 5. Acta Trop. 2012. PMID: 21382335 Free PMC article. Review.
Cited by
-
Malaria in Cambodia: A Retrospective Analysis of a Changing Epidemiology 2006-2019.Int J Environ Res Public Health. 2021 Feb 18;18(4):1960. doi: 10.3390/ijerph18041960. Int J Environ Res Public Health. 2021. PMID: 33670471 Free PMC article.
-
Market Formation in a Global Health Transition.Environ Innov Soc Transit. 2021 Sep;40:40-59. doi: 10.1016/j.eist.2021.05.003. Environ Innov Soc Transit. 2021. PMID: 35106274 Free PMC article.
-
Assessing the role of the for-profit private healthcare sector in malaria elimination efforts in Bangladesh: a cross-sectional study of challenges and opportunities.BMC Public Health. 2024 Oct 25;24(1):2969. doi: 10.1186/s12889-024-20448-2. BMC Public Health. 2024. PMID: 39455950 Free PMC article.
-
Expanding malaria diagnosis and treatment in Lao PDR: lessons learned from a public-private mix initiative.Malar J. 2017 Nov 13;16(1):460. doi: 10.1186/s12936-017-2104-5. Malar J. 2017. PMID: 29132370 Free PMC article.
-
Improving malaria case management with artemisinin-based combination therapies and malaria rapid diagnostic tests in private medicine retail outlets in sub-Saharan Africa: A systematic review.PLoS One. 2024 Jul 29;19(7):e0286718. doi: 10.1371/journal.pone.0286718. eCollection 2024. PLoS One. 2024. PMID: 39074113 Free PMC article.
References
-
- WHO. Malaria Elimination Strategy in the Greater Mekong Subregion. Geneva: World Health Organization; 2015. http://iris.wpro.who.int/bitstream/handle/10665.1/10945/9789290617181_en.... Accessed 28 Mar 2017.
-
- WHO. Guidelines for the treatment of malaria. 3rd edition. Geneva: World Health Organization; 2015. http://apps.who.int/iris/bitstream/10665/162441/1/9789241549127_eng.pdf. Accessed 28 Mar 2017.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
