

Contribution of Autonomic Reflexes to the Hyperadrenergic State in Heart Failure
- PMID: 28424575
- PMCID: PMC5372354
- DOI: 10.3389/fnins.2017.00162
Contribution of Autonomic Reflexes to the Hyperadrenergic State in Heart Failure
Abstract
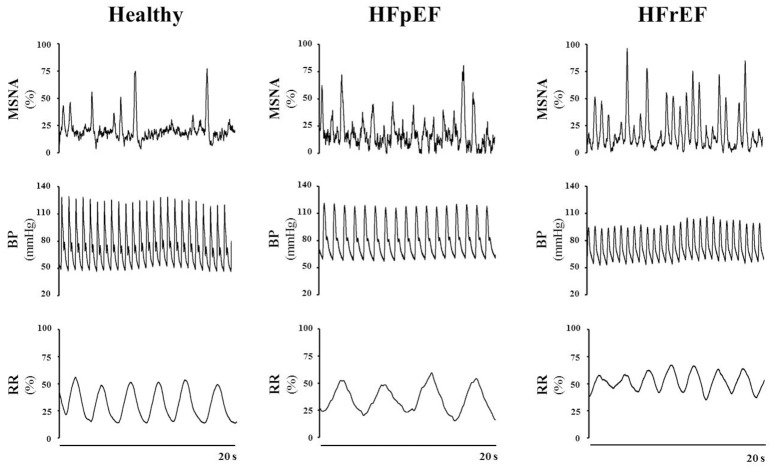
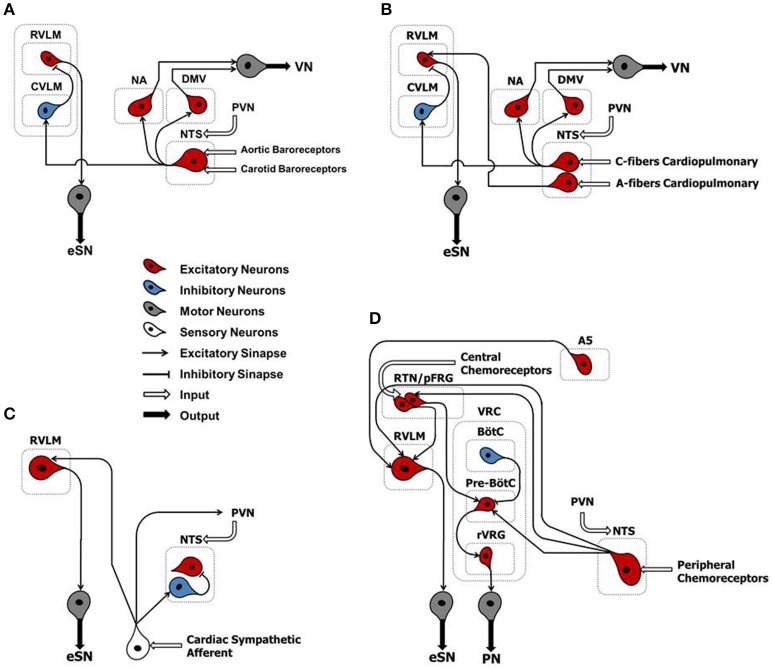
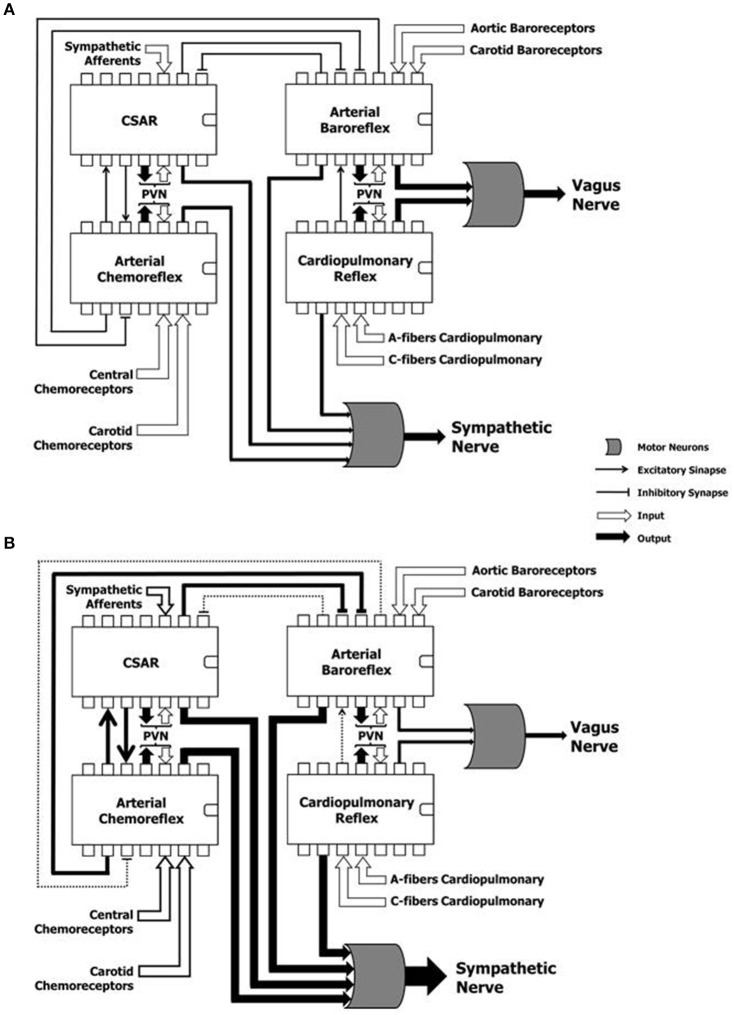
Heart failure (HF) is a complex syndrome representing the clinical endpoint of many cardiovascular diseases of different etiology. Given its prevalence, incidence and social impact, a better understanding of HF pathophysiology is paramount to implement more effective anti-HF therapies. Based on left ventricle (LV) performance, HF is currently classified as follows: (1) with reduced ejection fraction (HFrEF); (2) with mid-range EF (HFmrEF); and (3) with preserved EF (HFpEF). A central tenet of HFrEF pathophysiology is adrenergic hyperactivity, featuring increased sympathetic nerve discharge and a progressive loss of rhythmical sympathetic oscillations. The role of reflex mechanisms in sustaining adrenergic abnormalities during HFrEF is increasingly well appreciated and delineated. However, the same cannot be said for patients affected by HFpEF or HFmrEF, whom also present with autonomic dysfunction. Neural mechanisms of cardiovascular regulation act as "controller units," detecting and adjusting for changes in arterial blood pressure, blood volume, and arterial concentrations of oxygen, carbon dioxide and pH, as well as for humoral factors eventually released after myocardial (or other tissue) ischemia. They do so on a beat-to-beat basis. The central dynamic integration of all these afferent signals ensures homeostasis, at rest and during states of physiological or pathophysiological stress. Thus, the net result of information gathered by each controller unit is transmitted by the autonomic branch using two different codes: intensity and rhythm of sympathetic discharges. The main scope of the present article is to (i) review the key neural mechanisms involved in cardiovascular regulation; (ii) discuss how their dysfunction accounts for the hyperadrenergic state present in certain forms of HF; and (iii) summarize how sympathetic efferent traffic reveal central integration among autonomic mechanisms under physiological and pathological conditions, with a special emphasis on pathophysiological characteristics of HF.
Keywords: autonomic nervous system; cardiovascular variability; heart failure; sympathetic nerve activity.
Figures
Similar articles
-
Clinical characteristics and prognosis of heart failure with mid-range ejection fraction: insights from a multi-centre registry study in China.BMC Cardiovasc Disord. 2019 Sep 2;19(1):209. doi: 10.1186/s12872-019-1177-1. BMC Cardiovasc Disord. 2019. PMID: 31477021 Free PMC article.
-
[Contemporary epidemiology and treatment of hospitalized heart failure patients in real clinical practice in China].Zhonghua Xin Xue Guan Bing Za Zhi. 2019 Nov 24;47(11):865-874. doi: 10.3760/cma.j.issn.0253-3758.2019.11.004. Zhonghua Xin Xue Guan Bing Za Zhi. 2019. PMID: 31744275 Chinese.
-
Atrial Fibrillation in Heart Failure With Preserved, Mid-Range, and Reduced Ejection Fraction.JACC Heart Fail. 2017 Aug;5(8):565-574. doi: 10.1016/j.jchf.2017.05.001. Epub 2017 Jul 12. JACC Heart Fail. 2017. PMID: 28711451
-
Potential Role of the Retrotrapezoid Nucleus in Mediating Cardio-Respiratory Dysfunction in Heart Failure With Preserved Ejection Fraction.Front Physiol. 2022 Apr 12;13:863963. doi: 10.3389/fphys.2022.863963. eCollection 2022. Front Physiol. 2022. PMID: 35492622 Free PMC article. Review.
-
Research Opportunities in Autonomic Neural Mechanisms of Cardiopulmonary Regulation: A Report From the National Heart, Lung, and Blood Institute and the National Institutes of Health Office of the Director Workshop.JACC Basic Transl Sci. 2022 Jan 26;7(3):265-293. doi: 10.1016/j.jacbts.2021.11.003. eCollection 2022 Mar. JACC Basic Transl Sci. 2022. PMID: 35411324 Free PMC article. Review.
Cited by
-
Effect of SGLT2 Inhibitors on the Sympathetic Nervous System and Blood Pressure.Curr Cardiol Rep. 2019 Jun 21;21(8):70. doi: 10.1007/s11886-019-1165-1. Curr Cardiol Rep. 2019. PMID: 31227915 Review.
-
Absence of synemin in mice causes structural and functional abnormalities in heart.J Mol Cell Cardiol. 2018 Jan;114:354-363. doi: 10.1016/j.yjmcc.2017.12.005. Epub 2017 Dec 14. J Mol Cell Cardiol. 2018. PMID: 29247678 Free PMC article.
-
Sympathetic activation in heart failure with reduced and mildly reduced ejection fraction: the role of aetiology.ESC Heart Fail. 2021 Dec;8(6):5112-5120. doi: 10.1002/ehf2.13580. Epub 2021 Sep 7. ESC Heart Fail. 2021. PMID: 34492735 Free PMC article.
-
Arrhythmogenic Mechanisms in Heart Failure: Linking β-Adrenergic Stimulation, Stretch, and Calcium.Front Physiol. 2018 Oct 16;9:1453. doi: 10.3389/fphys.2018.01453. eCollection 2018. Front Physiol. 2018. PMID: 30374311 Free PMC article. Review.
-
Altered Heart Rate Turbulence and Variability Parameters Predict 1-Year Mortality in Heart Failure with Preserved Ejection Fraction.J Cardiovasc Dev Dis. 2022 Jul 2;9(7):213. doi: 10.3390/jcdd9070213. J Cardiovasc Dev Dis. 2022. PMID: 35877575 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous