

KRAS G12C mutation as a poor prognostic marker of pemetrexed treatment in non-small cell lung cancer
- PMID: 28407465
- PMCID: PMC5432792
- DOI: 10.3904/kjim.2015.299
KRAS G12C mutation as a poor prognostic marker of pemetrexed treatment in non-small cell lung cancer
Abstract
Background/aims: The predictive and prognostic value of KRAS mutation and its type of mutations in non-small cell lung cancer (NSCLC) are controversial. This clinical study was designed to investigate the predictive value of KRAS mutations and its mutation types to pemetrexed and gemcitabine based treatment.
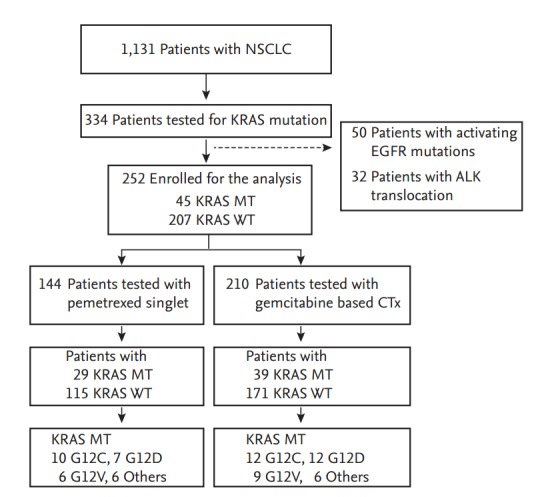
Methods: Advanced NSCLC patients tested for KRAS mutation (n = 334) were retrospectively reviewed and 252 patients with wild type epidermal growth factor receptor and no anaplastic lymphoma kinase fusion were enrolled for the analysis. KRAS mutations were observed in 45 subjects with mutation type as followed: G12C (n = 13), G12D (n = 12), G12V (n = 12), other (n = 8). Response rate (RR), progression-free survival (PFS), and overall survival (OS) of pemetrexed singlet and gemcitabine based chemotherapy were analysis.
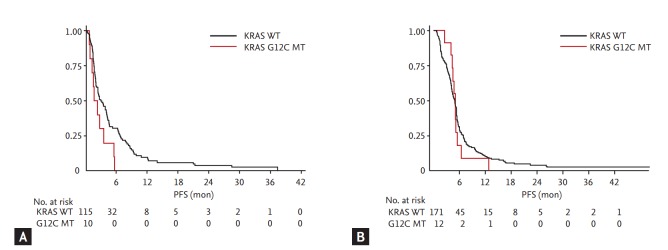
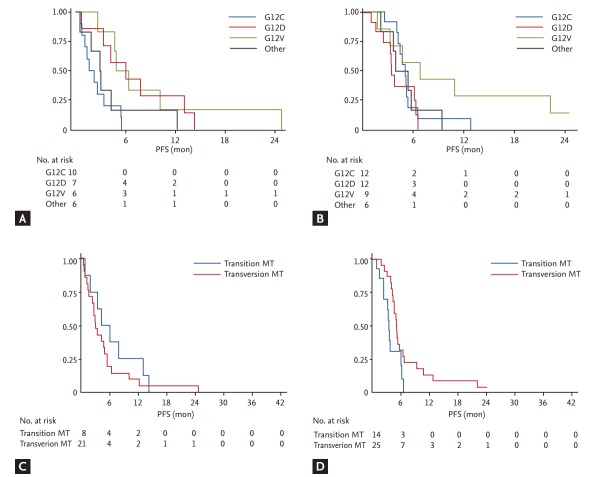
Results: Age, sex, performance status were well balanced between subjects with or without KRAS mutations. No difference was observed in RR. Hazard ratio (HR) of PFS for pemetrexed treated subjects with G12C mutation compared to subjects with KRAS wild type was 1.96 (95% confidential interval [CI], 1.01 to 3.79; p = 0.045), but other mutations failed to show clinical significance. By analysis done by PFS, compared to the subjects with transition mutation, HR was 1.48 (95% CI, 0.64 to 3.40; p = 0.360) for subjects with transversion mutation on pemetrexed treatment and 0.41 (95% CI, 0.19 to 0.87; p = 0.020) for subjects treated with gemcitabine based chemotherapy. No difference was observed in OS.
Conclusions: In this study, different drug sensitivity was observed according to the type of KRAS mutation. NSCLC subpopulations with different KRAS mutation type should be considered as different subgroups and optimal chemotherapy regimens should be searched in further confirmative studies.
Keywords: Carcinoma, non-small-cell lung; Gemcitabine; KRAS; Pemetrexed.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Realities of KRAS-mutated non-small cell lung cancer.Korean J Intern Med. 2017 May;32(3):442. doi: 10.3904/kjim.2017.148. Epub 2017 Apr 28. Korean J Intern Med. 2017. PMID: 28490719 Free PMC article. No abstract available.
Similar articles
-
Comparison of clinical outcome after first-line platinum-based chemotherapy in different types of KRAS mutated advanced non-small-cell lung cancer.Lung Cancer. 2015 Nov;90(2):249-54. doi: 10.1016/j.lungcan.2015.09.012. Epub 2015 Sep 15. Lung Cancer. 2015. PMID: 26415993
-
The prevalence and prognostic value of KRAS co-mutation subtypes in Chinese advanced non-small cell lung cancer patients.Cancer Med. 2020 Jan;9(1):84-93. doi: 10.1002/cam4.2682. Epub 2019 Nov 10. Cancer Med. 2020. PMID: 31709742 Free PMC article.
-
The prevalence and real-world therapeutic analysis of Chinese patients with KRAS-Mutant Non-Small Cell lung cancer.Cancer Med. 2022 Oct;11(19):3581-3592. doi: 10.1002/cam4.4739. Epub 2022 Apr 8. Cancer Med. 2022. PMID: 35394121 Free PMC article.
-
Bayesian network meta-comparison of maintenance treatments for stage IIIb/IV non-small-cell lung cancer (NSCLC) patients with good performance status not progressing after first-line induction chemotherapy: results by performance status, EGFR mutation, histology and response to previous induction.Eur J Cancer. 2015 Nov;51(16):2330-44. doi: 10.1016/j.ejca.2015.07.007. Epub 2015 Sep 10. Eur J Cancer. 2015. PMID: 26364517 Review.
-
Personalized medicine in non-small-cell lung cancer: is KRAS a useful marker in selecting patients for epidermal growth factor receptor-targeted therapy?J Clin Oncol. 2010 Nov 1;28(31):4769-77. doi: 10.1200/JCO.2009.27.4365. Epub 2010 Oct 4. J Clin Oncol. 2010. PMID: 20921461 Review.
Cited by
-
TTF-1 and EGFR expression are related to EGFR mutation in lung adenocarcinoma.Int J Clin Exp Pathol. 2018 Sep 1;11(9):4650-4656. eCollection 2018. Int J Clin Exp Pathol. 2018. PMID: 31949865 Free PMC article.
-
Notch Transduction in Non-Small Cell Lung Cancer.Int J Mol Sci. 2020 Aug 8;21(16):5691. doi: 10.3390/ijms21165691. Int J Mol Sci. 2020. PMID: 32784481 Free PMC article. Review.
-
Management of KRAS-Mutant Non-Small Cell Lung Cancer in the Era of Precision Medicine.Curr Treat Options Oncol. 2018 Jun 27;19(8):43. doi: 10.1007/s11864-018-0557-6. Curr Treat Options Oncol. 2018. PMID: 29951788 Review.
-
KRAS as a Prognostic and Predictive Marker in Metastatic Non-Small Cell Lung Carcinoma: A Systematic Review.Cureus. 2024 May 10;16(5):e60061. doi: 10.7759/cureus.60061. eCollection 2024 May. Cureus. 2024. PMID: 38860089 Free PMC article. Review.
-
Clinical outcomes to pemetrexed-based versus non-pemetrexed-based platinum doublets in patients with KRAS-mutant advanced non-squamous non-small cell lung cancer.Clin Transl Oncol. 2020 May;22(5):708-716. doi: 10.1007/s12094-019-02175-y. Epub 2019 Jul 22. Clin Transl Oncol. 2020. PMID: 31332704
References
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- Rosell R, Carcereny E, Gervais R, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012;13:239–246. - PubMed
-
- Solomon BJ, Mok T, Kim DW, et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N Engl J Med. 2014;371:2167–2177. - PubMed
-
- Suda K, Tomizawa K, Mitsudomi T. Biological and clinical significance of KRAS mutations in lung cancer: an oncogenic driver that contrasts with EGFR mutation. Cancer Metastasis Rev. 2010;29:49–60. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous