

The potential impact and cost of focusing HIV prevention on young women and men: A modeling analysis in western Kenya
- PMID: 28403211
- PMCID: PMC5389814
- DOI: 10.1371/journal.pone.0175447
The potential impact and cost of focusing HIV prevention on young women and men: A modeling analysis in western Kenya
Abstract
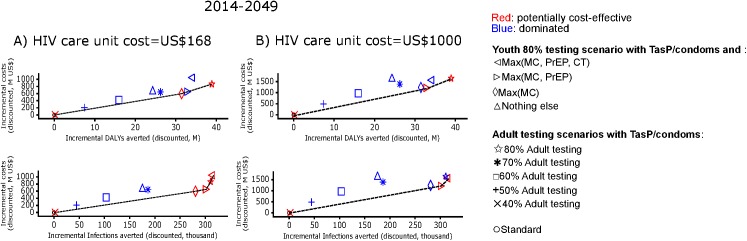
Objective: We compared the impact and costs of HIV prevention strategies focusing on youth (15-24 year-old persons) versus on adults (15+ year-old persons), in a high-HIV burden context of a large generalized epidemic.
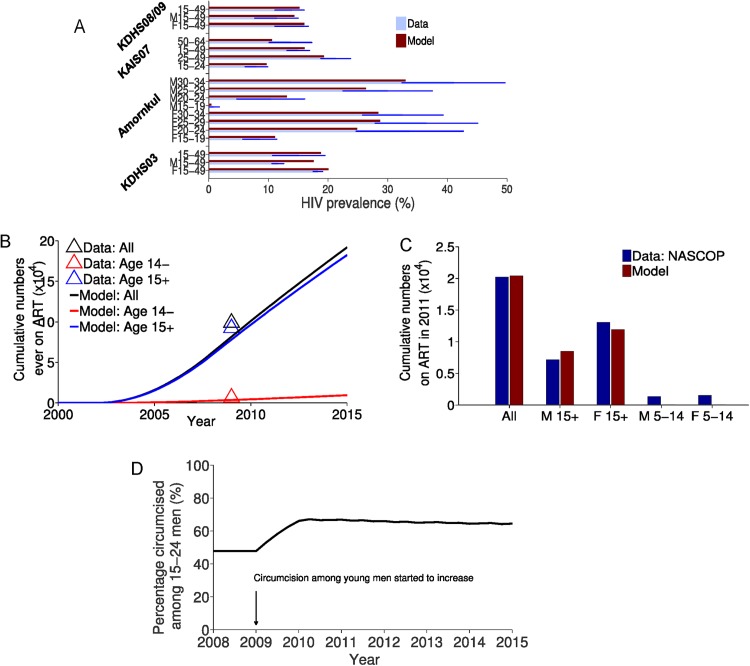
Design: Compartmental age-structured mathematical model of HIV transmission in Nyanza, Kenya.
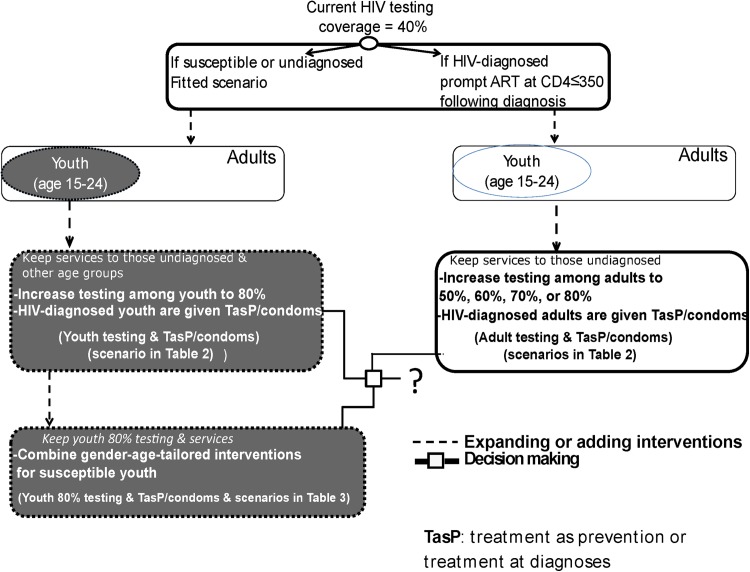
Interventions: The interventions focused on youth were high coverage HIV testing (80% of youth), treatment at diagnosis (TasP, i.e., immediate start of antiretroviral therapy [ART]) and 10% increased condom usage for HIV-positive diagnosed youth, male circumcision for HIV-negative young men, pre-exposure prophylaxis (PrEP) for high-risk HIV-negative females (ages 20-24 years), and cash transfer for in-school HIV-negative girls (ages 15-19 years). Permutations of these were compared to adult-focused HIV testing coverage with condoms and TasP.
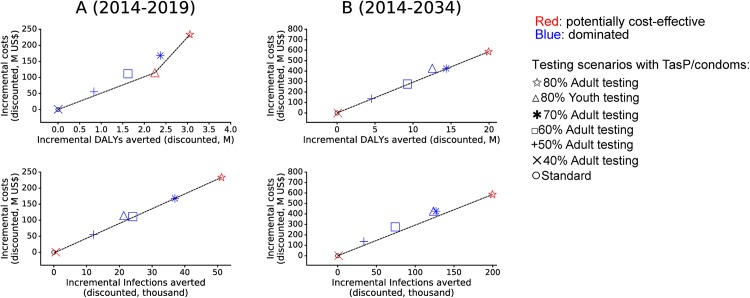
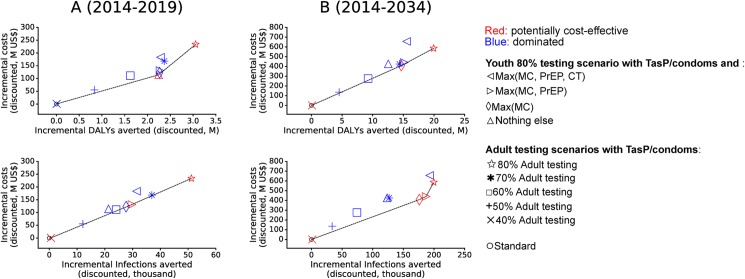
Results: The youth-focused strategy with ART treatment at diagnosis and condom use without adding interventions for HIV-negative youth performed better than the adult-focused strategy with adult testing reaching 50-60% coverage and TasP/condoms. Over the long term, the youth-focused strategy approached the performance of 70% adult testing and TasP/condoms. When high coverage male circumcision also is added to the youth-focused strategy, the combined intervention outperformed the adult-focused strategy with 70% testing, for at least 35 years by averting 94,000 more infections, averting 5.0 million more disability-adjusted life years (DALYs), and saving US$46.0 million over this period. The addition of prevention interventions beyond circumcision to the youth-focused strategy would be more beneficial if HIV care costs are high, or when program delivery costs are relatively high for programs encompassing HIV testing coverage exceeding 70%, TasP and condoms to HIV-infected adults compared to combination prevention programs among youth.
Conclusion: For at least the next three decades, focusing in high burden settings on high coverage HIV testing, ART treatment upon diagnosis, condoms and male circumcision among youth may outperform adult-focused ART treatment upon diagnosis programs, unless the adult testing coverage in these programs reaches very high levels (>70% of all adults reached) at similar program costs. Our results indicate the potential importance of age-targeting for HIV prevention in the current era of 'test and start, ending AIDS' goals to ameliorate the HIV epidemic globally.
Conflict of interest statement
Figures
Similar articles
-
Modelling the impact and cost-effectiveness of combination prevention amongst HIV serodiscordant couples in Nigeria.AIDS. 2015 Sep 24;29(15):2035-44. doi: 10.1097/QAD.0000000000000798. AIDS. 2015. PMID: 26355574 Free PMC article.
-
Understanding the potential impact of a combination HIV prevention intervention in a hyper-endemic community.PLoS One. 2013;8(1):e54575. doi: 10.1371/journal.pone.0054575. Epub 2013 Jan 23. PLoS One. 2013. PMID: 23372738 Free PMC article.
-
Evaluating the cost-effectiveness of pre-exposure prophylaxis (PrEP) and its impact on HIV-1 transmission in South Africa.PLoS One. 2010 Nov 5;5(11):e13646. doi: 10.1371/journal.pone.0013646. PLoS One. 2010. PMID: 21079767 Free PMC article.
-
Where to deploy pre-exposure prophylaxis (PrEP) in sub-Saharan Africa?Sex Transm Infect. 2013 Dec;89(8):628-34. doi: 10.1136/sextrans-2012-050891. Epub 2013 Aug 2. Sex Transm Infect. 2013. PMID: 23912819 Review.
-
Behavioral interventions to reduce risk for sexual transmission of HIV among men who have sex with men.Cochrane Database Syst Rev. 2008 Jul 16;(3):CD001230. doi: 10.1002/14651858.CD001230.pub2. Cochrane Database Syst Rev. 2008. PMID: 18646068 Review.
Cited by
-
Incremental costs of integrated PrEP provision and effective use counselling in community-based platforms for adolescent girls and young women in South Africa: an observational study.J Int AIDS Soc. 2022 Feb;25(2):e25875. doi: 10.1002/jia2.25875. J Int AIDS Soc. 2022. PMID: 35129299 Free PMC article. Clinical Trial.
-
Infectious Disease Modelling of HIV Prevention Interventions: A Systematic Review and Narrative Synthesis of Compartmental Models.Pharmacoeconomics. 2023 Jun;41(6):693-707. doi: 10.1007/s40273-023-01260-z. Epub 2023 Mar 29. Pharmacoeconomics. 2023. PMID: 36988896 Free PMC article.
-
The costs of scaling up HIV and syphilis testing in low- and middle-income countries: a systematic review.Health Policy Plan. 2021 Jun 25;36(6):939-954. doi: 10.1093/heapol/czab030. Health Policy Plan. 2021. PMID: 33693731 Free PMC article.
-
Lessons from a decade of voluntary medical male circumcision implementation and their application to HIV pre-exposure prophylaxis scale up.Int J STD AIDS. 2018 Dec;29(14):1432-1443. doi: 10.1177/0956462418787896. Epub 2018 Aug 16. Int J STD AIDS. 2018. PMID: 30114997 Free PMC article. Review.
-
Understanding the Evolving Role of Voluntary Medical Male Circumcision as a Public Health Strategy in Eastern and Southern Africa: Opportunities and Challenges.Curr HIV/AIDS Rep. 2022 Dec;19(6):526-536. doi: 10.1007/s11904-022-00639-5. Epub 2022 Dec 2. Curr HIV/AIDS Rep. 2022. PMID: 36459306 Free PMC article. Review.
References
-
- UNAIDS. 90–90–90—An ambitious treatment target to help end the AIDS epidemic | UNAIDS [Internet]. [cited 26 Dec 2016]. Available: http://www.unaids.org/en/resources/documents/2014/90-90-90
-
- Kasedde S, Luo C, McClure C, Chandan U. Reducing HIV and AIDS in adolescents: opportunities and challenges. Curr HIV/AIDS Rep. 2013;10: 159–168. doi: 10.1007/s11904-013-0159-7 - DOI - PubMed
-
- WHO. World Health Organization. Health for the World’s Adolescents: a Second Chance in the Second Decade, 2014. [Internet]. [cited 26 Dec 2016]. Available: http://apps.who.int/iris/bitstream/10665/112750/1/WHO_FWC_MCA_14.05_eng.pdf
-
- UNICEF. Home. In: Children and AIDS [Internet]. [cited 26 Dec 2016]. Available: http://childrenandaids.org/home
-
- Idele P, Gillespie A, Porth T, Suzuki C, Mahy M, Kasedde S, et al. Epidemiology of HIV and AIDS Among Adolescents: Current Status, Inequities, and Data Gaps. JAIDS J Acquir Immune Defic Syndr. 2014;66: S144–S153. doi: 10.1097/QAI.0000000000000176 - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
