

Colorectal Cancer Incidence Patterns in the United States, 1974-2013
- PMID: 28376186
- PMCID: PMC6059239
- DOI: 10.1093/jnci/djw322
Colorectal Cancer Incidence Patterns in the United States, 1974-2013
Abstract
Background: Colorectal cancer (CRC) incidence in the United States is declining rapidly overall but, curiously, is increasing among young adults. Age-specific and birth cohort patterns can provide etiologic clues, but have not been recently examined.
Methods: CRC incidence trends in Surveillance, Epidemiology, and End Results areas from 1974 to 2013 (n = 490 305) were analyzed by five-year age group and birth cohort using incidence rate ratios (IRRs) and age-period-cohort modeling.
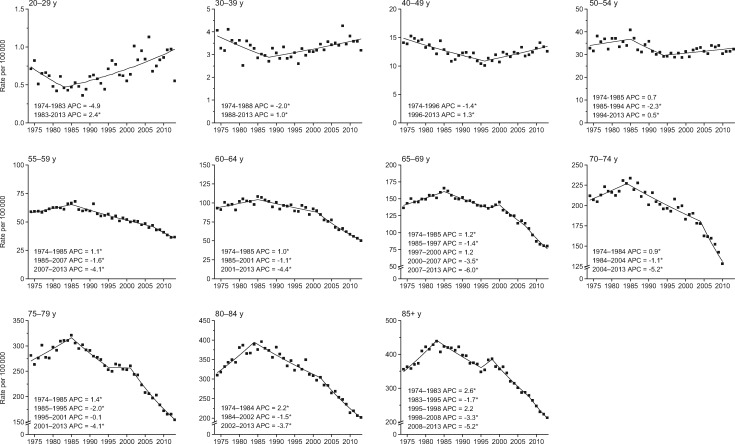
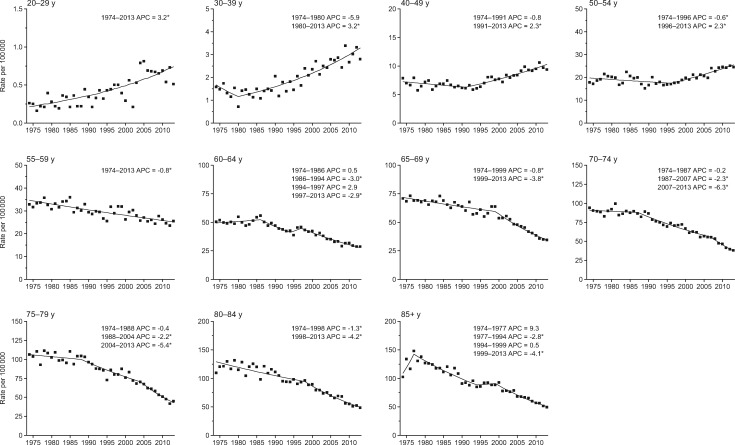
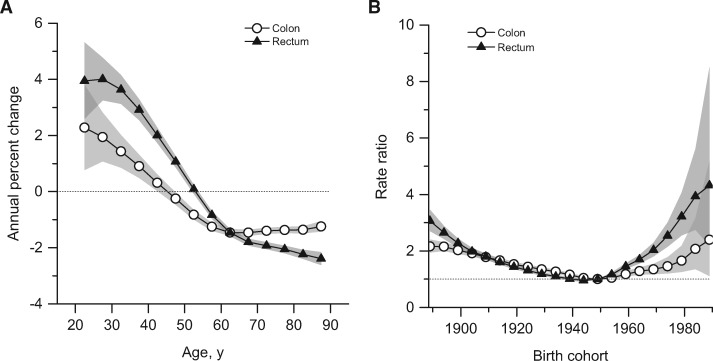
Results: After decreasing in the previous decade, colon cancer incidence rates increased by 1.0% to 2.4% annually since the mid-1980s in adults age 20 to 39 years and by 0.5% to 1.3% since the mid-1990s in adults age 40 to 54 years; rectal cancer incidence rates have been increasing longer and faster (eg, 3.2% annually from 1974-2013 in adults age 20-29 years). In adults age 55 years and older, incidence rates generally declined since the mid-1980s for colon cancer and since 1974 for rectal cancer. From 1989-1990 to 2012-2013, rectal cancer incidence rates in adults age 50 to 54 years went from half those in adults age 55 to 59 to equivalent (24.7 vs 24.5 per 100 000 persons: IRR = 1.01, 95% confidence interval [CI] = 0.92 to 1.10), and the proportion of rectal cancer diagnosed in adults younger than age 55 years doubled from 14.6% (95% CI = 14.0% to 15.2%) to 29.2% (95% CI = 28.5% to 29.9%). Age-specific relative risk by birth cohort declined from circa 1890 until 1950, but continuously increased through 1990. Consequently, compared with adults born circa 1950, those born circa 1990 have double the risk of colon cancer (IRR = 2.40, 95% CI = 1.11 to 5.19) and quadruple the risk of rectal cancer (IRR = 4.32, 95% CI = 2.19 to 8.51).
Conclusions: Age-specific CRC risk has escalated back to the level of those born circa 1890 for contemporary birth cohorts, underscoring the need for increased awareness among clinicians and the general public, as well as etiologic research to elucidate causes for the trend. Further, as nearly one-third of rectal cancer patients are younger than age 55 years, screening initiation before age 50 years should be considered.
© The Author 2017. Published by Oxford University Press. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Response.J Natl Cancer Inst. 2017 Aug 1;109(8):djx100. doi: 10.1093/jnci/djx100. J Natl Cancer Inst. 2017. PMID: 29117389 Free PMC article. No abstract available.
-
RE: Colorectal Cancer Incidence Patterns in the United States, 1974-2013.J Natl Cancer Inst. 2017 Aug 1;109(8). doi: 10.1093/jnci/djx103. J Natl Cancer Inst. 2017. PMID: 29117390 No abstract available.
-
RE: Colorectal Cancer Incidence Patterns in the United States, 1974-2013.J Natl Cancer Inst. 2017 Aug 1;109(8):djx104. doi: 10.1093/jnci/djx104. J Natl Cancer Inst. 2017. PMID: 29117391 Free PMC article. No abstract available.
Similar articles
-
Increasing disparities in the age-related incidences of colon and rectal cancers in the United States, 1975-2010.JAMA Surg. 2015 Jan;150(1):17-22. doi: 10.1001/jamasurg.2014.1756. JAMA Surg. 2015. PMID: 25372703 Free PMC article.
-
Colorectal cancer statistics, 2017.CA Cancer J Clin. 2017 May 6;67(3):177-193. doi: 10.3322/caac.21395. Epub 2017 Mar 1. CA Cancer J Clin. 2017. PMID: 28248415
-
Contributions of Adenocarcinoma and Carcinoid Tumors to Early-Onset Colorectal Cancer Incidence Rates in the United States.Ann Intern Med. 2021 Feb;174(2):157-166. doi: 10.7326/M20-0068. Epub 2020 Dec 15. Ann Intern Med. 2021. PMID: 33315473
-
Epidemiology and Mechanisms of the Increasing Incidence of Colon and Rectal Cancers in Young Adults.Gastroenterology. 2020 Jan;158(2):341-353. doi: 10.1053/j.gastro.2019.07.055. Epub 2019 Aug 5. Gastroenterology. 2020. PMID: 31394082 Free PMC article. Review.
-
Rectal Cancer in Asian vs. Western Countries: Why the Variation in Incidence?Curr Treat Options Oncol. 2017 Sep 25;18(10):64. doi: 10.1007/s11864-017-0500-2. Curr Treat Options Oncol. 2017. PMID: 28948490 Review.
Cited by
-
Canadian Colorectal Cancer Screening Guidelines: Do They Need an Update Given Changing Incidence and Global Practice Patterns?Curr Oncol. 2021 Apr 21;28(3):1558-1570. doi: 10.3390/curroncol28030147. Curr Oncol. 2021. PMID: 33919428 Free PMC article. Review.
-
Assessing the Role of Flexible Sigmoidoscopy for Patients With Positive Fecal Immunochemical Test (FIT) and Rectal Bleeding as a Sole Symptom Within the Fast-Track Pathway.Cureus. 2024 Sep 10;16(9):e69060. doi: 10.7759/cureus.69060. eCollection 2024 Sep. Cureus. 2024. PMID: 39391448 Free PMC article.
-
Utility of machine learning in developing a predictive model for early-age-onset colorectal neoplasia using electronic health records.PLoS One. 2022 Mar 10;17(3):e0265209. doi: 10.1371/journal.pone.0265209. eCollection 2022. PLoS One. 2022. PMID: 35271664 Free PMC article.
-
Disease Burden of Total and Early-Onset Colorectal Cancer in China from 1990 to 2019 and Predictions of Cancer Incidence and Mortality.Clin Epidemiol. 2023 Feb 1;15:151-163. doi: 10.2147/CLEP.S391058. eCollection 2023. Clin Epidemiol. 2023. PMID: 36755975 Free PMC article.
-
Transmission and clearance of potential procarcinogenic bacteria during fecal microbiota transplantation for recurrent Clostridioides difficile.JCI Insight. 2019 Oct 3;4(19):e130848. doi: 10.1172/jci.insight.130848. JCI Insight. 2019. PMID: 31578306 Free PMC article.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;661:7–30. - PubMed
-
- Welch HG, Robertson DJ. Colorectal cancer on the decline—why screening can’t explain it all. N Engl J Med. 2016;37417:1605–1607. - PubMed
-
- O’Connell JB, Maggard MA, Liu JH, Etzioni DA, Livingston EH, Ko CY. Rates of colon and rectal cancers are increasing in young adults. Am Surg. 2003;6910:866–872. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
