

Personalizing the Intensity of Blood Pressure Control: Modeling the Heterogeneity of Risks and Benefits From SPRINT (Systolic Blood Pressure Intervention Trial)
- PMID: 28373269
- PMCID: PMC5428922
- DOI: 10.1161/CIRCOUTCOMES.117.003624
Personalizing the Intensity of Blood Pressure Control: Modeling the Heterogeneity of Risks and Benefits From SPRINT (Systolic Blood Pressure Intervention Trial)
Abstract
Background: In SPRINT (Systolic Blood Pressure Intervention Trial), patients with hypertension and high cardiovascular risk treated with intensive blood pressure (BP) control (<120 mm Hg) had fewer major adverse cardiovascular events (MACE) and deaths but higher rates of treatment-related serious adverse events (SAE) than patients randomized to standard BP control (<140 mm Hg). However, the degree of benefit or harm for an individual patient could vary because of heterogeneity in treatment effect.
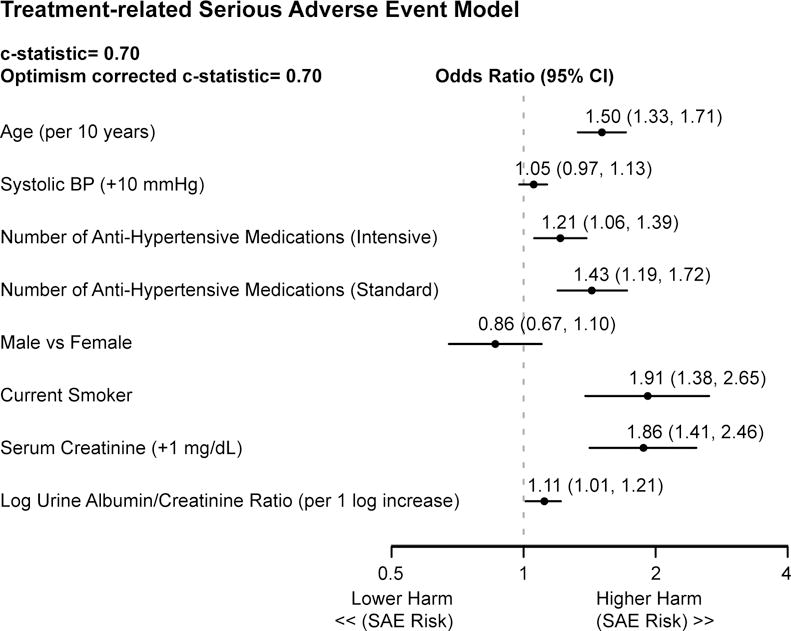
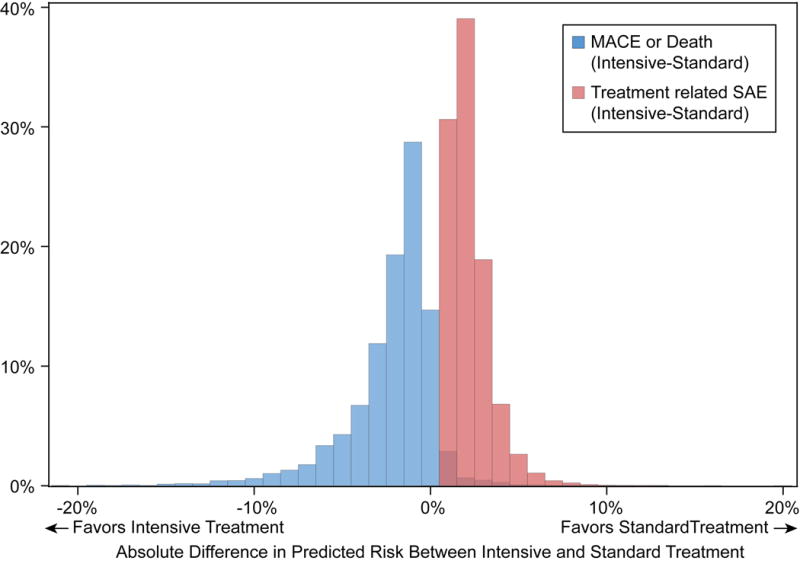
Methods and results: Using patient-level data from 9361 randomized patients in SPRINT, we developed models to predict risk for MACE or death and treatment-related SAE to allow for individualized BP treatment goals based on each patient's projected risk and benefit of intensive versus standard BP control. Models were internally validated using bootstrap resampling and externally validated on 4741 patients from the ACCORD-BP (The Action to Control Cardiovascular Risk in Diabetes blood pressure) trial. Among 9361 SPRINT patients, 755 patients (8.1%) had a MACE or death event and 338 patients (3.6%) had a treatment-related SAE during a median follow-up of 3.3 years. The MACE/death and the SAE model had C statistics of 0.72 and 0.70, respectively, in the derivation cohort and 0.69 and 0.65 in ACCORD. The MACE/death model had 10 variables including treatment interactions with age, baseline systolic BP, and diastolic BP, and the SAE model had 8 variables including treatment interaction with number of BP medications. Intensive BP treatment was associated with a mean 2.2±2.6% lower risk of MACE/death compared with standard treatment (range, 20.7% lower risk to 19.6% greater risk among individual patients) and a mean 2.2±1.2% higher risk for SAEs (range, 0.5%-15.8% more harm in individual patients).
Conclusions: To translate the findings from SPRINT to clinical practice, we developed prediction models to tailor the intensity of BP control based on the projected risk and benefit for each unique patient. This approach should be prospectively tested to better engage patients in shared medical decision making and to improve outcomes.
Clinical trial registration: URL: https://clinicaltrials.gov. Unique identifier: NCT01206062.
Keywords: acute kidney injury; adult; blood pressure; decision making; hypertension.
© 2017 American Heart Association, Inc.
Conflict of interest statement
Figures

Similar articles
-
Benefit and harm of intensive blood pressure treatment: Derivation and validation of risk models using data from the SPRINT and ACCORD trials.PLoS Med. 2017 Oct 17;14(10):e1002410. doi: 10.1371/journal.pmed.1002410. eCollection 2017 Oct. PLoS Med. 2017. PMID: 29040268 Free PMC article. Clinical Trial.
-
Effect of Intensive Blood Pressure Treatment on Heart Failure Events in the Systolic Blood Pressure Reduction Intervention Trial.Circ Heart Fail. 2017 Apr;10(4):e003613. doi: 10.1161/CIRCHEARTFAILURE.116.003613. Circ Heart Fail. 2017. PMID: 28364091 Free PMC article. Clinical Trial.
-
Clinical Value of Predicting Individual Treatment Effects for Intensive Blood Pressure Therapy.Circ Cardiovasc Qual Outcomes. 2019 Mar;12(3):e005010. doi: 10.1161/CIRCOUTCOMES.118.005010. Circ Cardiovasc Qual Outcomes. 2019. Retraction in: Circ Cardiovasc Qual Outcomes. 2023 Oct;16(10):e000119. doi: 10.1161/HCQ.0000000000000119 PMID: 30857410 Free PMC article. Retracted.
-
Treatment of Hypertension: Which Goal for Which Patient?Adv Exp Med Biol. 2017;956:117-127. doi: 10.1007/5584_2016_97. Adv Exp Med Biol. 2017. PMID: 27722961 Review.
-
Should blood pressure goal be individualized in hypertensive patients?Pharmacol Res. 2017 Apr;118:53-63. doi: 10.1016/j.phrs.2016.11.037. Epub 2016 Dec 2. Pharmacol Res. 2017. PMID: 27919826 Review.
Cited by
-
Which Target Blood Pressure in Year 2018? Evidence from Recent Clinical Trials.High Blood Press Cardiovasc Prev. 2018 Jun;25(2):151-158. doi: 10.1007/s40292-018-0258-z. Epub 2018 Apr 16. High Blood Press Cardiovasc Prev. 2018. PMID: 29663195 Review.
-
Systolic inter-arm blood pressure difference and risk of cognitive decline in older people: a cohort study.Br J Gen Pract. 2020 Jun 25;70(696):e472-e480. doi: 10.3399/bjgp20X709589. Print 2020 Jul. Br J Gen Pract. 2020. PMID: 32366532 Free PMC article.
-
Individualising intensive systolic blood pressure reduction in hypertension using computational trial phenomaps and machine learning: a post-hoc analysis of randomised clinical trials.Lancet Digit Health. 2022 Nov;4(11):e796-e805. doi: 10.1016/S2589-7500(22)00170-4. Lancet Digit Health. 2022. PMID: 36307193 Free PMC article. Clinical Trial.
-
Personalized prediction of adverse heart and kidney events using baseline and longitudinal data from SPRINT and ACCORD.PLoS One. 2019 Aug 8;14(8):e0219728. doi: 10.1371/journal.pone.0219728. eCollection 2019. PLoS One. 2019. PMID: 31393900 Free PMC article.
-
Estimated Population Health Benefits of Intensive Systolic Blood Pressure Treatment Among SPRINT-Eligible US Adults.Am J Hypertens. 2023 Aug 5;36(9):498-508. doi: 10.1093/ajh/hpad047. Am J Hypertens. 2023. PMID: 37378472 Free PMC article.
References
-
- Wright JT, Jr, Williamson JD, Whelton PK, Snyder JK, Sink KM, Rocco MV, Reboussin DM, Rahman M, Oparil S, Lewis CE, Kimmel PL, Johnson KC, Goff DC, Jr, Fine LJ, Cutler JA, Cushman WC, Cheung AK, Ambrosius WT. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N Engl J Med. 2015;373:2103–16. - PMC - PubMed
-
- Ambrosius WT, Sink KM, Foy CG, Berlowitz DR, Cheung AK, Cushman WC, Fine LJ, Goff DC, Jr, Johnson KC, Killeen AA, Lewis CE, Oparil S, Reboussin DM, Rocco MV, Snyder JK, Williamson JD, Wright JT, Jr, Whelton PK. The design and rationale of a multicenter clinical trial comparing two strategies for control of systolic blood pressure: the Systolic Blood Pressure Intervention Trial (SPRINT) Clin Trials. 2014;11:532–46. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
