

Cytomegalovirus duodenitis associated with life-threatening duodenal hemorrhage in an immunocompetent patient: A case report
- PMID: 28292662
- PMCID: PMC5348597
- DOI: 10.1016/j.ijscr.2017.02.029
Cytomegalovirus duodenitis associated with life-threatening duodenal hemorrhage in an immunocompetent patient: A case report
Abstract
Introduction: Cytomegalovirus (CMV) is known to be opportunistic in immunocompromised patients. However, there have been emerging cases of severe CMV infections found in immunocompetent patients. Gastrointestinal (GI) CMV disease is the most common manifestation affecting immunocompetent patients, with duodenal involvement being exceedingly rare. Presented is a case of an immunocompetent patient with life-threatening bleeding caused by CMV duodenitis, requiring surgical intervention.
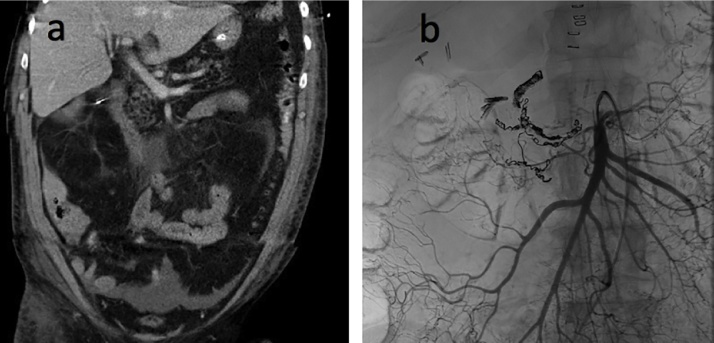
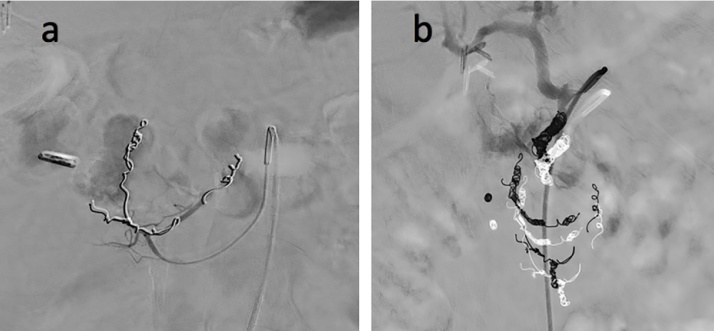
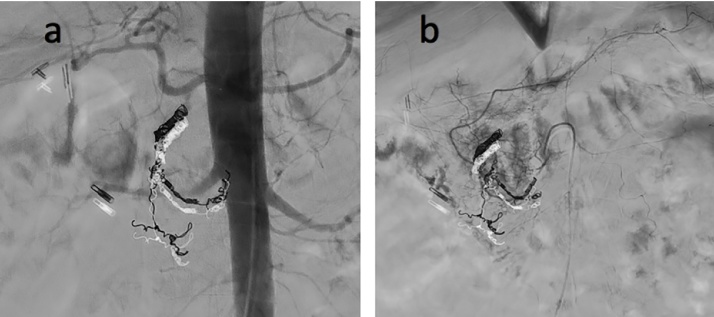
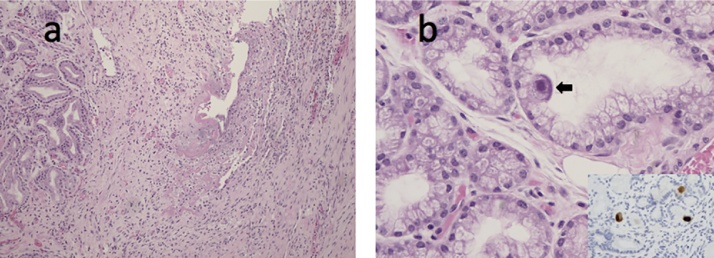
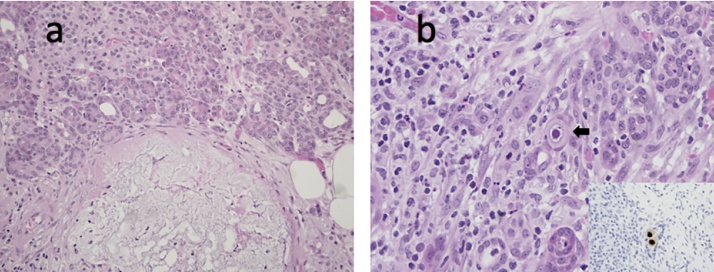
Presentation of case: A 60-year-old male with history of disseminated Methicillin-sensitive Staphylococcus aureus (MSSA) bacteremia and aortic valve infective endocarditis, presented with life-threatening upper GI hemorrhage. Endoscopy revealed ulcerations, with associated generalized mucosal bleeding in the duodenum. After repeated endoscopic therapies and failed interventional-radiology arterial embolization, the patient required a duodenectomy and associated total pancreatectomy, to control the duodenal hemorrhage. Pathologic review of the surgical specimen demonstrated CMV duodenitis. Systemic ganciclovir was utilized postoperatively.
Discussion: GI CMV infections should be on the differential diagnosis of immunocompetent patients presenting with uncontrollable GI bleeding, especially in critically ill patients due to transiently suppressed immunity. Endoscopic and histopathological examinations are often required for diagnosis. Ganciclovir is first-line treatment. Surgical intervention may be considered if there is recurrent bleeding and CMV duodenitis is suspected because of high potential for bleeding-associated mortality.
Conclusion: Presented is a rare case of life-threatening GI hemorrhage caused by CMV duodenitis in an immunocompetent patient. The patient failed endoscopic and interventional-radiology treatment options, and ultimately stabilized after surgical intervention.
Keywords: Cytomegalovirus; Duodenitis; Duodenum; Enteritis; Gastrointestinal bleed; Immunocompetent.
Copyright © 2017 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures
Similar articles
-
Lower gastrointestinal bleeding due to cytomegalovirus ileal ulcers in an immunocompetent man.Yonsei Med J. 2001 Feb;42(1):147-51. doi: 10.3349/ymj.2001.42.1.147. Yonsei Med J. 2001. PMID: 11293496
-
CMV enteritis causing massive intestinal hemorrhage in an elderly patient.Case Rep Med. 2010;2010:385795. doi: 10.1155/2010/385795. Epub 2010 Jul 12. Case Rep Med. 2010. PMID: 20706684 Free PMC article.
-
Symptomatic CMV duodenitis. An important clinical problem in AIDS.J Clin Gastroenterol. 1992 Jun;14(4):293-7. J Clin Gastroenterol. 1992. PMID: 1318892
-
Reactivated cytomegalovirus proctitis in an immunocompetent patient presenting as nosocomial diarrhea: a case report and literature review.BMC Infect Dis. 2017 Feb 1;17(1):113. doi: 10.1186/s12879-017-2218-y. BMC Infect Dis. 2017. PMID: 28143418 Free PMC article. Review.
-
Cytomegalovirus related fatal duodenal diverticular bleeding: Case report and literature review.World J Gastroenterol. 2016 Aug 21;22(31):7166-74. doi: 10.3748/wjg.v22.i31.7166. World J Gastroenterol. 2016. PMID: 27610026 Free PMC article. Review.
Cited by
-
Life-threatening gastrointestinal bleeding caused by cytomegalovirus-induced duodenal ulcer in a patient with AIDS: A case report.Heliyon. 2024 Apr 20;10(9):e30112. doi: 10.1016/j.heliyon.2024.e30112. eCollection 2024 May 15. Heliyon. 2024. PMID: 38737287 Free PMC article.
-
Programmed death-1 expression and regulatory T cells increase in the Intestinal mucosa of cytomegalovirus colitis in patients with HIV/AIDS.AIDS Res Ther. 2020 Sep 5;17(1):54. doi: 10.1186/s12981-020-00315-x. AIDS Res Ther. 2020. PMID: 32891157 Free PMC article.
-
Cytomegalovirus cell tropism and clinicopathological characteristics in gastrointestinal tract of patients with HIV/AIDS.Diagn Pathol. 2022 Jan 14;17(1):9. doi: 10.1186/s13000-022-01193-9. Diagn Pathol. 2022. PMID: 35027044 Free PMC article.
-
Cytomegalovirus Ileitis in a Patient With Post-severe Trauma: A Case Report.In Vivo. 2024 Sep-Oct;38(5):2562-2564. doi: 10.21873/invivo.13731. In Vivo. 2024. PMID: 39187352 Free PMC article.
-
Cytomegalovirus Disease of the Upper Gastrointestinal Tract: An Emerging Infection in Immunocompetent Hosts.GE Port J Gastroenterol. 2017 Nov;24(6):259-261. doi: 10.1159/000479974. Epub 2017 Aug 31. GE Port J Gastroenterol. 2017. PMID: 29255765 Free PMC article. No abstract available.
References
-
- Kalil A.C., Florescu D.F. Prevalence and mortality associated with cytomegalovirus infection in nonimmunosuppressed patients in the intensive care unit. Crit. Care Med. 2009;37(8):2350–2358. - PubMed
-
- You D.M., Johnson M.D. Cytomegalovirus infection and the gastrointestinal tract. Curr. Gastroenterol. Rep. 2012;14(4):334–342. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
