

Electrical neuromodulation of the cervical spinal cord facilitates forelimb skilled function recovery in spinal cord injured rats
- PMID: 28192079
- PMCID: PMC6219872
- DOI: 10.1016/j.expneurol.2017.02.006
Electrical neuromodulation of the cervical spinal cord facilitates forelimb skilled function recovery in spinal cord injured rats
Abstract
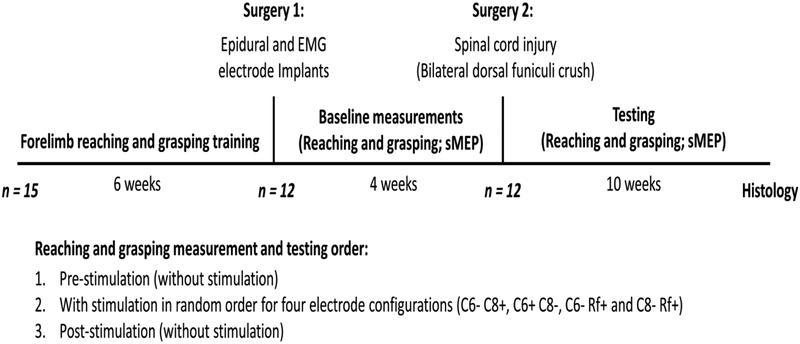
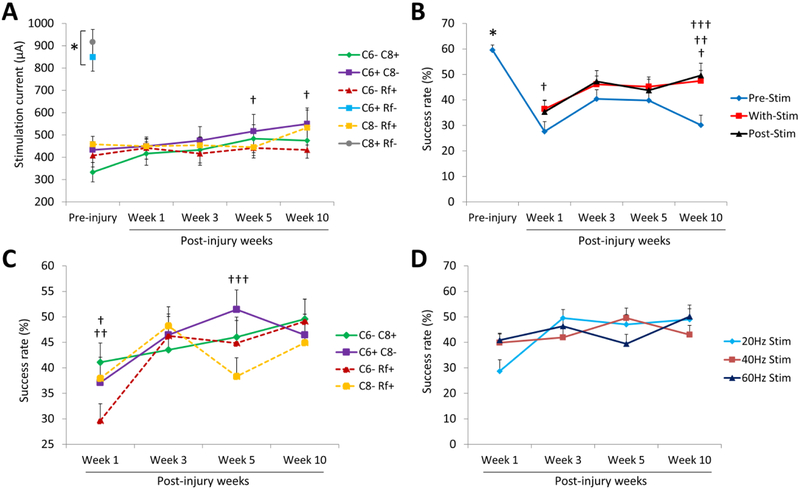
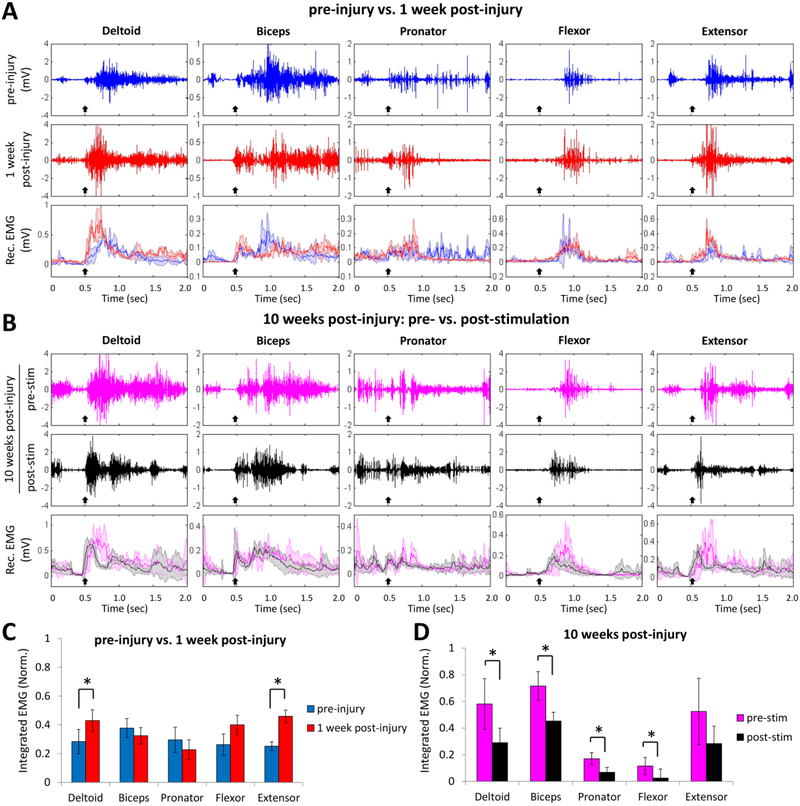
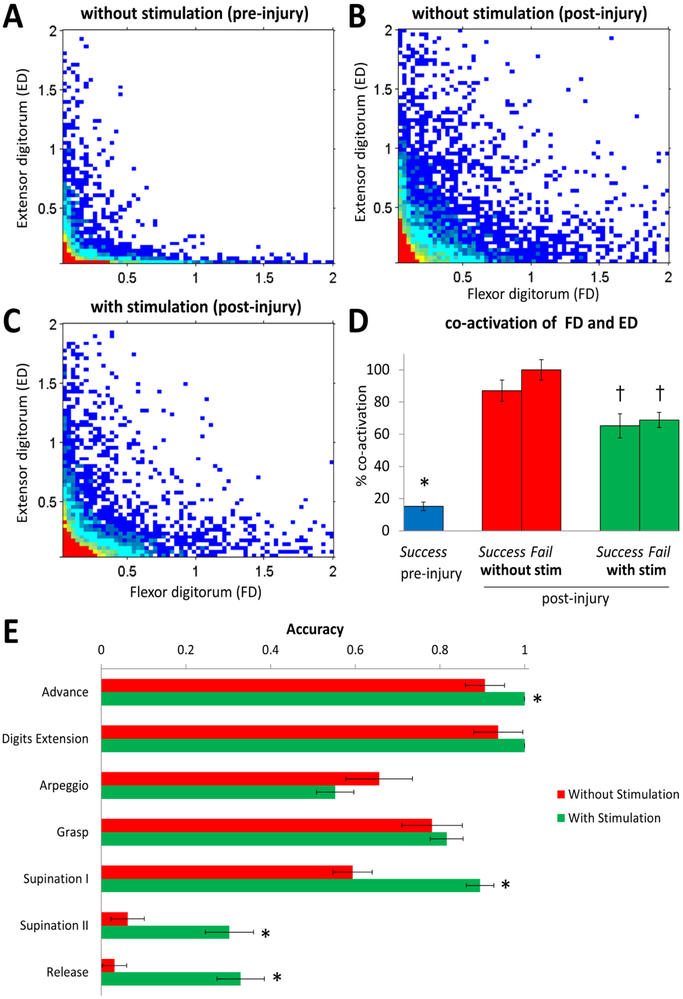
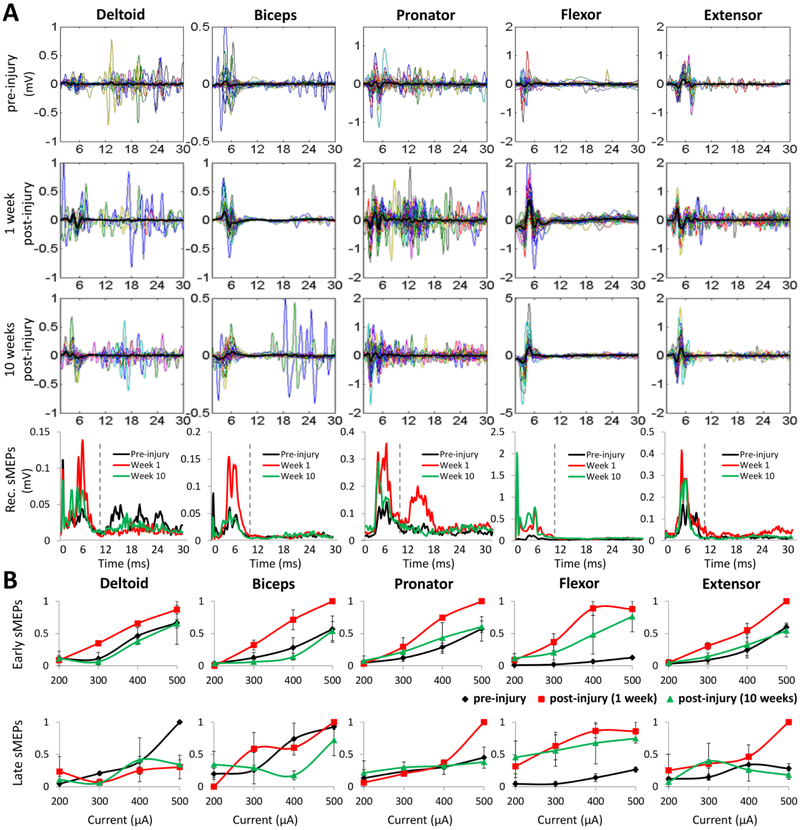
Enabling motor control by epidural electrical stimulation of the spinal cord is a promising therapeutic technique for the recovery of motor function after a spinal cord injury (SCI). Although epidural electrical stimulation has resulted in improvement in hindlimb motor function, it is unknown whether it has any therapeutic benefit for improving forelimb fine motor function after a cervical SCI. We tested whether trains of pulses delivered at spinal cord segments C6 and C8 would facilitate the recovery of forelimb fine motor control after a cervical SCI in rats. Rats were trained to reach and grasp sugar pellets. Immediately after a dorsal funiculus crush at C4, the rats showed significant deficits in forelimb fine motor control. The rats were tested to reach and grasp with and without cervical epidural stimulation for 10weeks post-injury. To determine the best stimulation parameters to activate the cervical spinal networks involved in forelimb motor function, monopolar and bipolar currents were delivered at varying frequencies (20, 40, and 60Hz) concomitant with the reaching and grasping task. We found that cervical epidural stimulation increased reaching and grasping success rates compared to the no stimulation condition. Bipolar stimulation (C6- C8+ and C6+ C8-) produced the largest spinal motor-evoked potentials (sMEPs) and resulted in higher reaching and grasping success rates compared with monopolar stimulation (C6- Ref+ and C8- Ref+). Forelimb performance was similar when tested at stimulation frequencies of 20, 40, and 60Hz. We also found that the EMG activity in most forelimb muscles as well as the co-activation between flexor and extensor muscles increased post-injury. With epidural stimulation, however, this trend was reversed indicating that cervical epidural spinal cord stimulation has therapeutic potential for rehabilitation after a cervical SCI.
Keywords: Cervical spinal cord injury; Corticospinal tract; Epidural electrical stimulation; Motor-evoked potentials; Reaching and grasping.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest
V. Reggie Edgerton, Roland R. Roy and Yury Gerasimenko – researchers on the study team hold shareholder interest in NeuroRecovery Technologies. Drs. Edgerton, Roy, Lu and Gerasimenko also hold certain inventorship rights on intellectual property licensed by The Regents of the University of California to NeuroRecovery Technologies and its subsidiaries.
Figures
Similar articles
-
Evaluation of optimal electrode configurations for epidural spinal cord stimulation in cervical spinal cord injured rats.J Neurosci Methods. 2015 May 30;247:50-7. doi: 10.1016/j.jneumeth.2015.03.012. Epub 2015 Mar 16. J Neurosci Methods. 2015. PMID: 25791014 Free PMC article.
-
Motor cortex and spinal cord neuromodulation promote corticospinal tract axonal outgrowth and motor recovery after cervical contusion spinal cord injury.Exp Neurol. 2017 Nov;297:179-189. doi: 10.1016/j.expneurol.2017.08.004. Epub 2017 Aug 10. Exp Neurol. 2017. PMID: 28803750 Free PMC article.
-
Serotonergic Facilitation of Forelimb Functional Recovery in Rats with Cervical Spinal Cord Injury.Neurotherapeutics. 2021 Apr;18(2):1226-1243. doi: 10.1007/s13311-020-00974-8. Epub 2021 Jan 8. Neurotherapeutics. 2021. PMID: 33420588 Free PMC article.
-
Prolonged acute intermittent hypoxia improves forelimb reach-to-grasp function in a rat model of chronic cervical spinal cord injury.Exp Neurol. 2021 Jun;340:113672. doi: 10.1016/j.expneurol.2021.113672. Epub 2021 Feb 27. Exp Neurol. 2021. PMID: 33652030 Review.
-
Electrical stimulation and motor recovery.Cell Transplant. 2015;24(3):429-46. doi: 10.3727/096368915X686904. Epub 2015 Feb 2. Cell Transplant. 2015. PMID: 25646771 Review.
Cited by
-
Asteroid impact: the potential of astrocytes to modulate human neural networks within organoids.Front Neurosci. 2023 Nov 22;17:1305921. doi: 10.3389/fnins.2023.1305921. eCollection 2023. Front Neurosci. 2023. PMID: 38075269 Free PMC article. Review.
-
Experimental spinal cord injury and behavioral tests in laboratory rats.Heliyon. 2019 Mar 8;5(3):e01324. doi: 10.1016/j.heliyon.2019.e01324. eCollection 2019 Mar. Heliyon. 2019. PMID: 30906898 Free PMC article. Review.
-
Non-invasive brain-spine interface: Continuous control of trans-spinal magnetic stimulation using EEG.Front Bioeng Biotechnol. 2022 Oct 31;10:975037. doi: 10.3389/fbioe.2022.975037. eCollection 2022. Front Bioeng Biotechnol. 2022. PMID: 36394044 Free PMC article.
-
When Spinal Neuromodulation Meets Sensorimotor Rehabilitation: Lessons Learned From Animal Models to Regain Manual Dexterity After a Spinal Cord Injury.Front Rehabil Sci. 2021 Dec 7;2:755963. doi: 10.3389/fresc.2021.755963. eCollection 2021. Front Rehabil Sci. 2021. PMID: 36188826 Free PMC article. Review.
-
Restoring Sensorimotor Function Through Neuromodulation After Spinal Cord Injury: Progress and Remaining Challenges.Front Neurosci. 2021 Oct 14;15:749465. doi: 10.3389/fnins.2021.749465. eCollection 2021. Front Neurosci. 2021. PMID: 34720867 Free PMC article. Review.
References
-
- Alam M, Rodrigues W, Pham BN, Thakor NV (2016) Brain-machine interface facilitated neurorehabilitation via spinal stimulation after spinal cord injury: Recent progress and future perspectives. Brain Research 1646:25–33. - PubMed
-
- Alstermark B, Isa T (2012) Circuits for Skilled Reaching and Grasping. Annual Review of Neuroscience 35:559–578. - PubMed
-
- Anderson KD (2004) Targeting recovery: priorities of the spinal cord-injured population. J Neurotrauma 21:1371–1383. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
