

Risk factors for surgical site infection following nonshunt pediatric neurosurgery: a review of 9296 procedures from a national database and comparison with a single-center experience
- PMID: 28186476
- PMCID: PMC5450913
- DOI: 10.3171/2016.11.PEDS16454
Risk factors for surgical site infection following nonshunt pediatric neurosurgery: a review of 9296 procedures from a national database and comparison with a single-center experience
Abstract
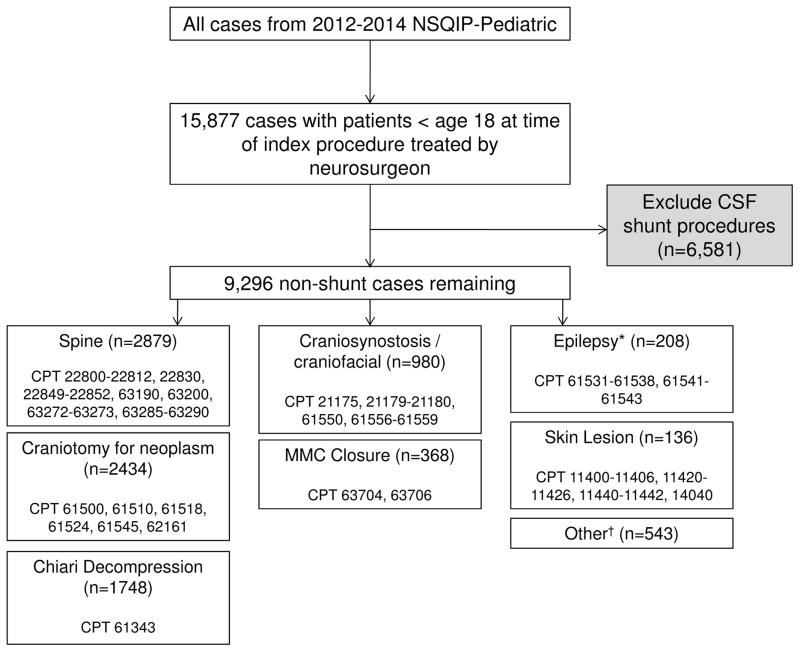
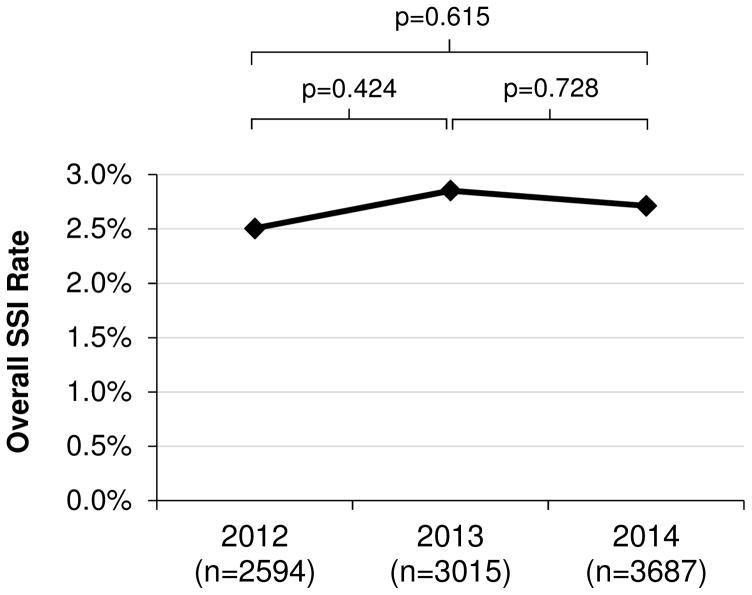
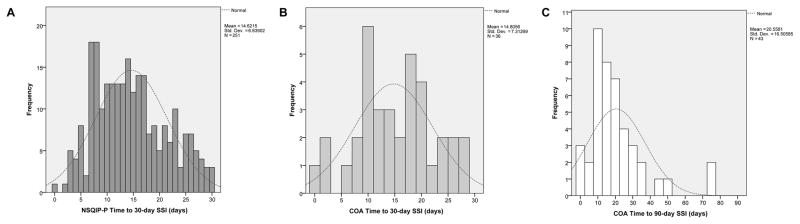
OBJECTIVE Surgical site infection (SSI) following CSF shunt operations has been well studied, yet risk factors for nonshunt pediatric neurosurgery are less well understood. The purpose of this study was to determine SSI rates and risk factors following nonshunt pediatric neurosurgery using a nationwide patient cohort and an institutional data set specifically for better understanding SSI. METHODS The authors reviewed the American College of Surgeons National Surgical Quality Improvement Program-Pediatric (ACS NSQIP-P) database for the years 2012-2014, including all neurosurgical procedures performed on pediatric patients except CSF shunts and hematoma evacuations. SSI included deep (intracranial abscesses, meningitis, osteomyelitis, and ventriculitis) and superficial wound infections. The authors performed univariate analyses of SSI association with procedure, demographic, comorbidity, operative, and hospital variables, with subsequent multivariate logistic regression analysis to determine independent risk factors for SSI within 30 days of the index procedure. A similar analysis was performed using a detailed institutional infection database from Children's of Alabama (COA). RESULTS A total of 9296 nonshunt procedures were identified in NSQIP-P with an overall 30-day SSI rate of 2.7%. The 30-day SSI rate in the COA institutional database was similar (3.3% of 1103 procedures, p = 0.325). Postoperative time to SSI in NSQIP-P and COA was 14.6 ± 6.8 days and 14.8 ± 7.3 days, respectively (mean ± SD). Myelomeningocele (4.3% in NSQIP-P, 6.3% in COA), spine (3.5%, 4.9%), and epilepsy (3.4%, 3.1%) procedure categories had the highest SSI rates by procedure category in both NSQIP-P and COA. Independent SSI risk factors in NSQIP-P included postoperative pneumonia (OR 4.761, 95% CI 1.269-17.857, p = 0.021), immune disease/immunosuppressant use (OR 3.671, 95% CI 1.371-9.827, p = 0.010), cerebral palsy (OR 2.835, 95% CI 1.463-5.494, p = 0.002), emergency operation (OR 1.843, 95% CI 1.011-3.360, p = 0.046), spine procedures (OR 1.673, 95% CI 1.036-2.702, p = 0.035), acquired CNS abnormality (OR 1.620, 95% CI 1.085-2.420, p = 0.018), and female sex (OR 1.475, 95% CI 1.062-2.049, p = 0.021). The only COA factor independently associated with SSI in the COA database included clean-contaminated wound classification (OR 3.887, 95% CI 1.354-11.153, p = 0.012), with public insurance (OR 1.966, 95% CI 0.957-4.041, p = 0.066) and spine procedures (OR 1.982, 95% CI 0.955-4.114, p = 0.066) approaching significance. Both NSQIP-P and COA multivariate model C-statistics were > 0.7. CONCLUSIONS The NSQIP-P SSI rates, but not risk factors, were similar to data from a single center.
Keywords: ACS = American College of Surgeons; AUC = area under the curve; COA = Children's of Alabama; CPT = Current Procedural Terminology; MMC = myelomeningocele; NSQIP; NSQIP = National Surgical Quality Improvement Program; NSQIP-P = NSQIP-Pediatric; ROC = receiver operating characteristic; SSI = surgical site infection; complication; pediatric neurosurgery; surgical site infection.
Conflict of interest statement
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures
Similar articles
-
Morbidity associated with 30-day surgical site infection following nonshunt pediatric neurosurgery.J Neurosurg Pediatr. 2017 Apr;19(4):421-427. doi: 10.3171/2016.11.PEDS16455. Epub 2017 Feb 10. J Neurosurg Pediatr. 2017. PMID: 28186474 Free PMC article.
-
Risk factors for unplanned readmission within 30 days after pediatric neurosurgery: a nationwide analysis of 9799 procedures from the American College of Surgeons National Surgical Quality Improvement Program.J Neurosurg Pediatr. 2016 Sep;18(3):350-62. doi: 10.3171/2016.2.PEDS15604. Epub 2016 May 17. J Neurosurg Pediatr. 2016. PMID: 27184348 Free PMC article.
-
Perioperative outcomes for pediatric neurosurgical procedures: analysis of the National Surgical Quality Improvement Program-Pediatrics.J Neurosurg Pediatr. 2017 Mar;19(3):361-371. doi: 10.3171/2016.10.PEDS16414. Epub 2017 Jan 6. J Neurosurg Pediatr. 2017. PMID: 28059679
-
Thirty-day readmission rates in spine surgery: systematic review and meta-analysis.Neurosurg Focus. 2015 Oct;39(4):E7. doi: 10.3171/2015.7.FOCUS1534. Neurosurg Focus. 2015. PMID: 26424347 Review.
-
Factors predictive of the development of surgical site infection in thyroidectomy - An analysis of NSQIP database.Int J Surg. 2018 Dec;60:273-278. doi: 10.1016/j.ijsu.2018.11.013. Epub 2018 Nov 16. Int J Surg. 2018. PMID: 30453084 Review.
Cited by
-
Length of preoperative hospital stay is the dominating risk factor for surgical site infection in neurosurgery: A cohort data-driven analysis.Surg Neurol Int. 2022 Mar 4;13:80. doi: 10.25259/SNI_1237_2021. eCollection 2022. Surg Neurol Int. 2022. PMID: 35399909 Free PMC article.
-
Thirty-day outcomes in pediatric epilepsy surgery.Childs Nerv Syst. 2018 Mar;34(3):487-494. doi: 10.1007/s00381-017-3639-z. Epub 2017 Oct 30. Childs Nerv Syst. 2018. PMID: 29086075
-
Venous thromboembolism following inpatient pediatric surgery: Analysis of 153,220 patients.J Pediatr Surg. 2019 Apr;54(4):631-639. doi: 10.1016/j.jpedsurg.2018.09.017. Epub 2018 Oct 10. J Pediatr Surg. 2019. PMID: 30361075 Free PMC article.
-
Longitudinal Analysis of Risk Factors for Clinical Outcomes of Enterobacteriaceae Meningitis/Encephalitis in Post-Neurosurgical Patients: A Comparative Cohort Study During 2014-2019.Infect Drug Resist. 2020 Jul 6;13:2161-2170. doi: 10.2147/IDR.S252331. eCollection 2020. Infect Drug Resist. 2020. PMID: 32753912 Free PMC article.
-
Surgical site infections after pediatric open airway reconstruction-A National Surgical Quality Improvement Program-Pediatric analysis.Laryngoscope Investig Otolaryngol. 2022 Aug 20;7(5):1618-1625. doi: 10.1002/lio2.895. eCollection 2022 Oct. Laryngoscope Investig Otolaryngol. 2022. PMID: 36258868 Free PMC article.
References
-
- Abdullah KG, Attiah MA, Olsen AS, Richardson A, Lucas TH. Reducing surgical site infections following craniotomy: examination of the use of topical vancomycin. J Neurosurg. 2015;123:1600–1604. - PubMed
-
- Abu Hamdeh S, Lytsy B, Ronne-Engström E. Surgical site infections in standard neurosurgery procedures- a study of incidence, impact and potential risk factors. Br J Neurosurg. 2014;28:270–275. - PubMed
-
- American College of Surgeons. User Guide for the 2012 ACS NSQIP Pediatric Participant Use Data File. Chicago: American College of Surgeons; 2013. [Accessed December 15, 2016]. ( https://www.facs.org/~/media/files/quality%20programs/nsqip/2012pedsuser...)
-
- American College of Surgeons. User Guide for the 2013 ACS NSQIP Pediatric Participant Use Data File. Chicago: American College of Surgeons; 2014. [Accessed December 15, 2016]. ( https://www.facs.org/~/media/files/quality%20programs/nsqip/peds_puf_use...)
-
- American College of Surgeons. User Guide for the 2014 ACS NSQIP Pediatric Participant Use Data File. Chicago: American College of Surgeons; 2015. [Accessed December 15, 2016]. ( https://www.facs.org/~/media/files/quality%20programs/nsqip/peds_acs_nsq...)
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
