

Large family cohorts of lymphoblastoid cells provide a new cellular model for investigating facioscapulohumeral muscular dystrophy
- PMID: 28161093
- PMCID: PMC5815870
- DOI: 10.1016/j.nmd.2016.12.007
Large family cohorts of lymphoblastoid cells provide a new cellular model for investigating facioscapulohumeral muscular dystrophy
Abstract
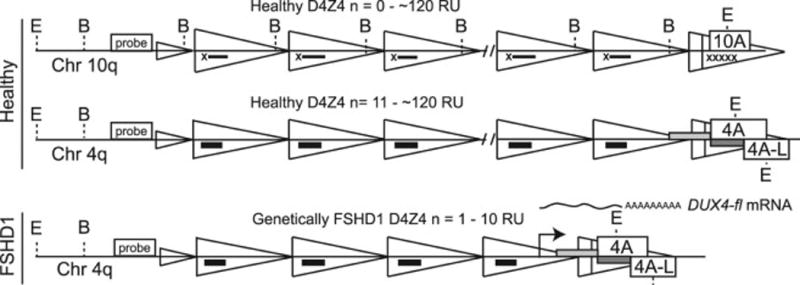
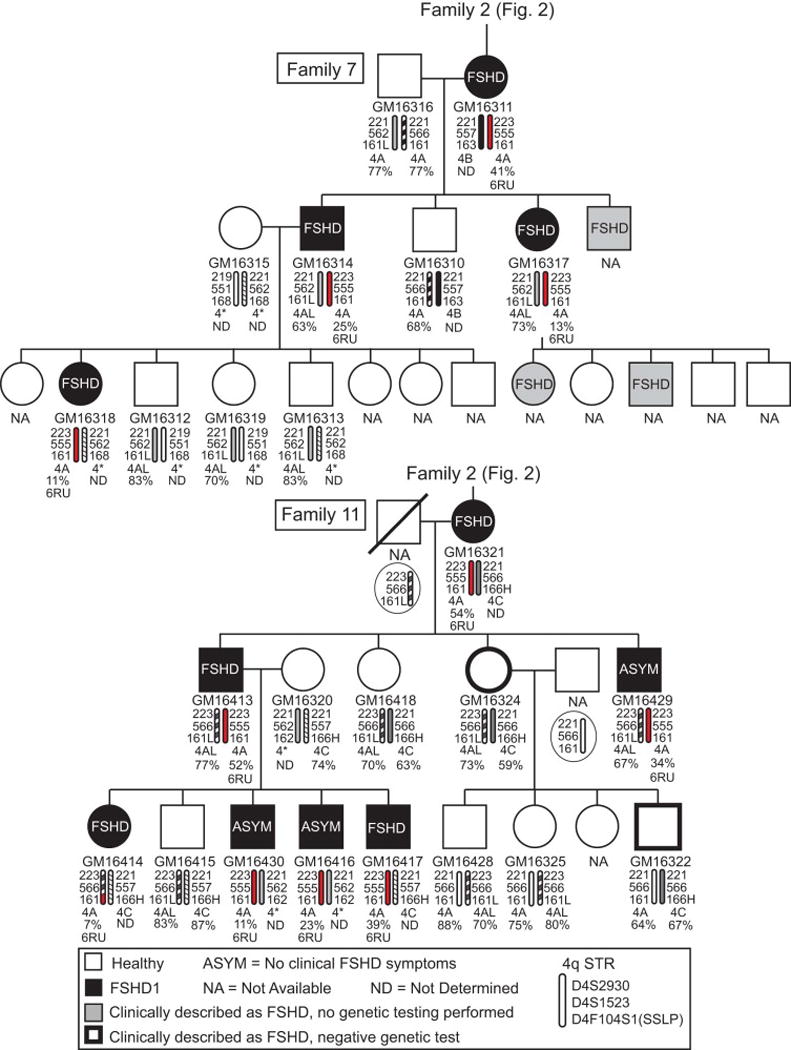
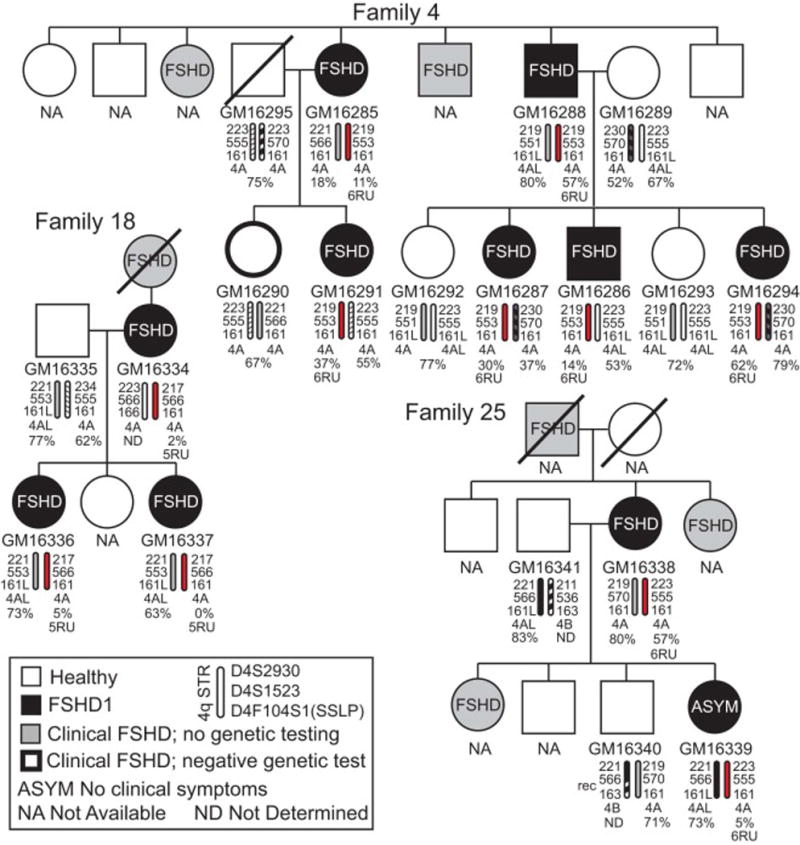
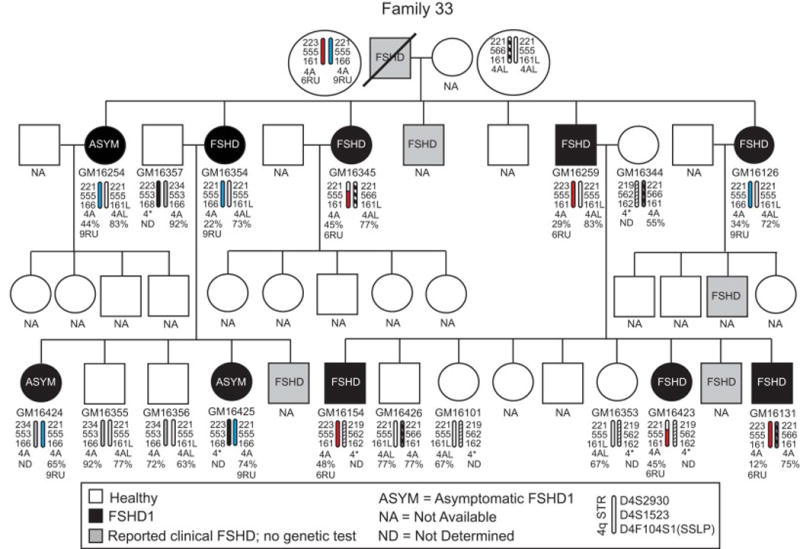
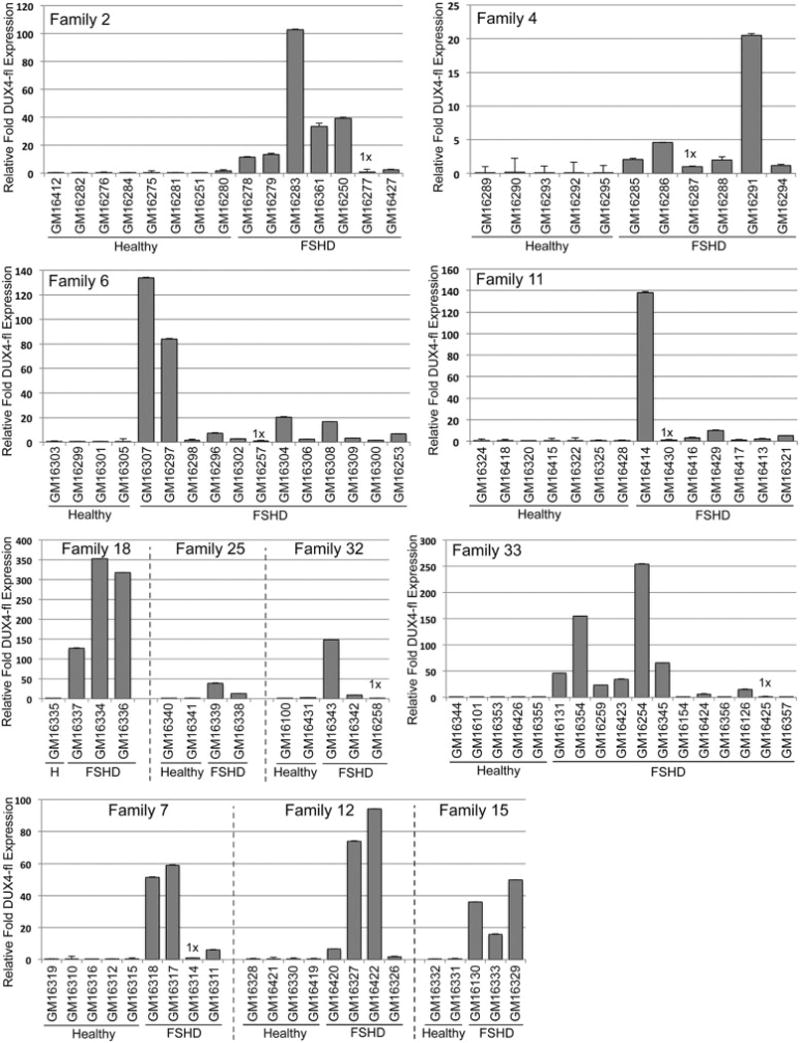
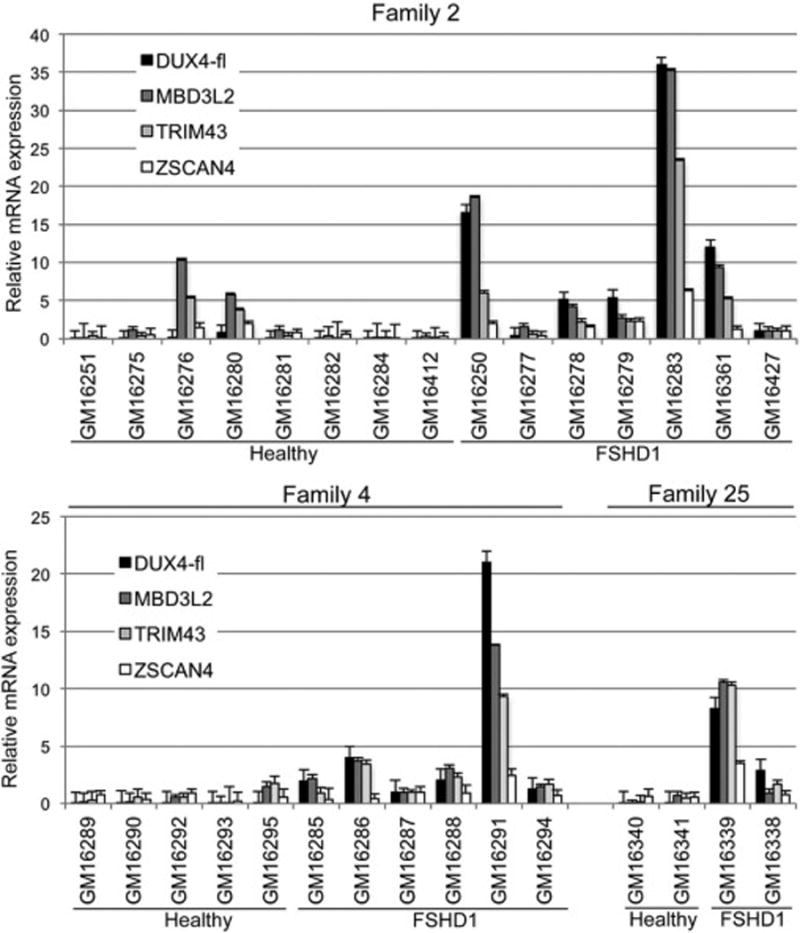
Facioscapulohumeral muscular dystrophy (FSHD) is associated with aberrant epigenetic regulation of the chromosome 4q35 D4Z4 macrosatellite repeat. The resulting DNA hypomethylation and relaxation of epigenetic repression leads to increased expression of the deleterious DUX4-fl mRNA encoded within the distal D4Z4 repeat. With the typical late onset of muscle weakness, prevalence of asymptomatic individuals, and an autosomal dominant mode of inheritance, FSHD is often passed on from one generation to the next and affects multiple individuals within a family. Here we have characterized unique collections of 114 lymphoblastoid cell lines (LCLs) generated from 12 multigenerational FSHD families, including 56 LCLs from large, genetically homogeneous families in Utah. We found robust expression of DUX4-fl in most FSHD LCLs and a good correlation between DNA hypomethylation and repeat length. In addition, DUX4-fl levels can be manipulated using epigenetic drugs as in myocytes, suggesting that some epigenetic pathways regulating DUX4-fl in myocytes are maintained in LCLs. Overall, these FSHD LCLs provide an alternative cellular model in which to study many aspects of D4Z4, DUX4, and FSHD gene regulation in a background of low genetic variation. Significantly, these non-adherent immortal LCLs are amenable for high-throughput screening of potential therapeutics targeting DUX4-fl mRNA or protein expression.
Keywords: D4Z4; DNA methylation; DUX4; Disease model; Epigenetic; FSHD.
Copyright © 2016 The Authors. Published by Elsevier B.V. All rights reserved.
Figures




Similar articles
-
Individual epigenetic status of the pathogenic D4Z4 macrosatellite correlates with disease in facioscapulohumeral muscular dystrophy.Clin Epigenetics. 2015 Mar 29;7(1):37. doi: 10.1186/s13148-015-0072-6. eCollection 2015. Clin Epigenetics. 2015. PMID: 25904990 Free PMC article.
-
Sporadic DUX4 expression in FSHD myocytes is associated with incomplete repression by the PRC2 complex and gain of H3K9 acetylation on the contracted D4Z4 allele.Epigenetics Chromatin. 2018 Aug 20;11(1):47. doi: 10.1186/s13072-018-0215-z. Epigenetics Chromatin. 2018. PMID: 30122154 Free PMC article.
-
Identification of Epigenetic Regulators of DUX4-fl for Targeted Therapy of Facioscapulohumeral Muscular Dystrophy.Mol Ther. 2018 Jul 5;26(7):1797-1807. doi: 10.1016/j.ymthe.2018.04.019. Epub 2018 Apr 26. Mol Ther. 2018. PMID: 29759937 Free PMC article.
-
A complex interplay of genetic and epigenetic events leads to abnormal expression of the DUX4 gene in facioscapulohumeral muscular dystrophy.Neuromuscul Disord. 2016 Dec;26(12):844-852. doi: 10.1016/j.nmd.2016.09.015. Epub 2016 Sep 19. Neuromuscul Disord. 2016. PMID: 27816329 Review.
-
Facioscapulohumeral muscular dystrophy: molecular pathological advances and future directions.Curr Opin Neurol. 2011 Oct;24(5):423-8. doi: 10.1097/WCO.0b013e32834959af. Curr Opin Neurol. 2011. PMID: 21734574 Review.
Cited by
-
Antagonism Between DUX4 and DUX4c Highlights a Pathomechanism Operating Through β-Catenin in Facioscapulohumeral Muscular Dystrophy.Front Cell Dev Biol. 2022 Sep 7;10:802573. doi: 10.3389/fcell.2022.802573. eCollection 2022. Front Cell Dev Biol. 2022. PMID: 36158201 Free PMC article.
-
Considerations and practical implications of performing a phenotypic CRISPR/Cas survival screen.PLoS One. 2022 Feb 17;17(2):e0263262. doi: 10.1371/journal.pone.0263262. eCollection 2022. PLoS One. 2022. PMID: 35176052 Free PMC article.
-
Transgenic mice expressing tunable levels of DUX4 develop characteristic facioscapulohumeral muscular dystrophy-like pathophysiology ranging in severity.Skelet Muscle. 2020 Apr 11;10(1):8. doi: 10.1186/s13395-020-00227-4. Skelet Muscle. 2020. PMID: 32278354 Free PMC article.
-
A cre-inducible DUX4 transgenic mouse model for investigating facioscapulohumeral muscular dystrophy.PLoS One. 2018 Feb 7;13(2):e0192657. doi: 10.1371/journal.pone.0192657. eCollection 2018. PLoS One. 2018. PMID: 29415061 Free PMC article.
-
Identification of candidate miRNA biomarkers for facioscapulohumeral muscular dystrophy using DUX4-based mouse models.Dis Model Mech. 2021 Aug 1;14(8):dmm049016. doi: 10.1242/dmm.049016. Epub 2021 Aug 24. Dis Model Mech. 2021. PMID: 34338285 Free PMC article.
References
-
- Padberg GW. Facioscapulohumeral Disease [thesis] Leiden University; Leiden, the Netherlands: 1982. p. 243.
-
- Flanigan KM. The muscular dystrophies. Semin Neurol. 2012;32:255–63. - PubMed
-
- Orphanet. Prevalence and incidence of rare diseases: Bibliographic data. Orphanet Report Series: Rare Diseases collection. 2016 [cited; Available from: http://www.orpha.net/orphacom/cahiers/docs/GB/Prevalence_of_rare_disease....
-
- Wang LH, Tawil R. Facioscapulohumeral Dystrophy. Curr Neurol Neurosci Rep. 2016;16:66. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
