

Sheet-Like Remodeling of the Transverse Tubular System in Human Heart Failure Impairs Excitation-Contraction Coupling and Functional Recovery by Mechanical Unloading
- PMID: 28073805
- PMCID: PMC5404964
- DOI: 10.1161/CIRCULATIONAHA.116.024470
Sheet-Like Remodeling of the Transverse Tubular System in Human Heart Failure Impairs Excitation-Contraction Coupling and Functional Recovery by Mechanical Unloading
Abstract
Background: Cardiac recovery in response to mechanical unloading by left ventricular assist devices (LVADs) has been demonstrated in subgroups of patients with chronic heart failure (HF). Hallmarks of HF are depletion and disorganization of the transverse tubular system (t-system) in cardiomyocytes. Here, we investigated remodeling of the t-system in human end-stage HF and its role in cardiac recovery.
Methods: Left ventricular biopsies were obtained from 5 donors and 26 patients with chronic HF undergoing implantation of LVADs. Three-dimensional confocal microscopy and computational image analysis were applied to assess t-system structure, density, and distance of ryanodine receptor clusters to the sarcolemma, including the t-system. Recovery of cardiac function in response to mechanical unloading was assessed by echocardiography during turndown of the LVAD.
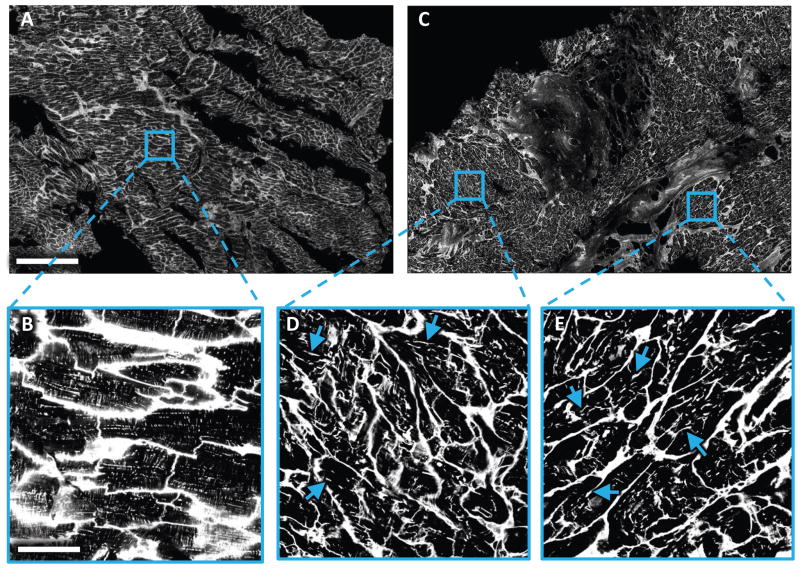
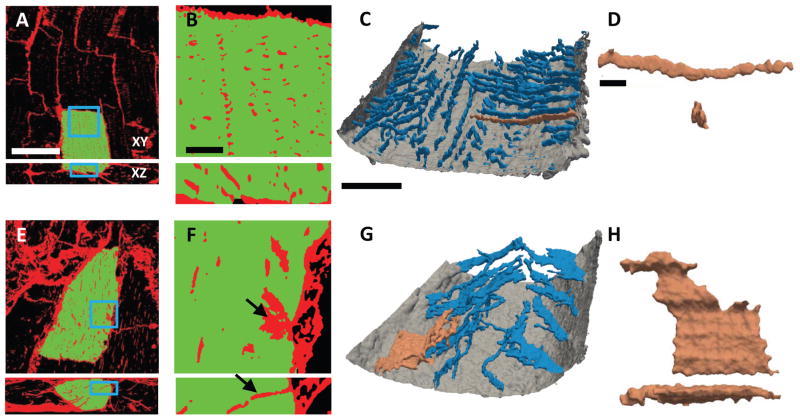
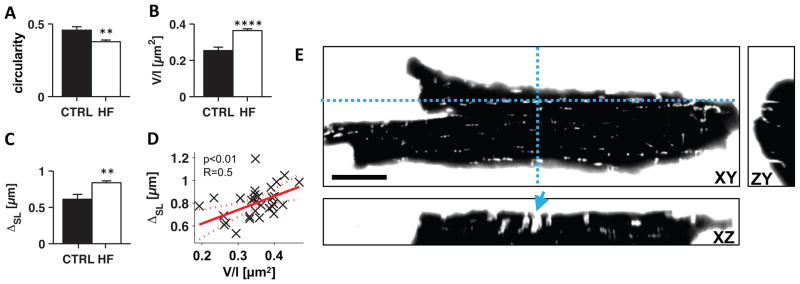
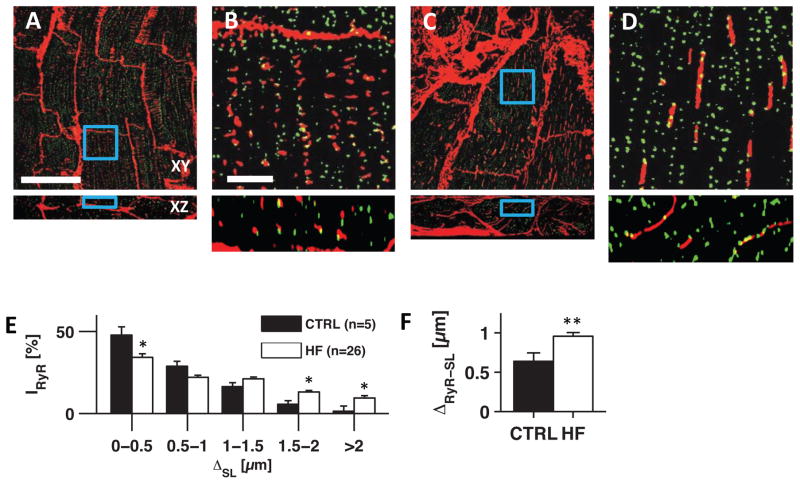
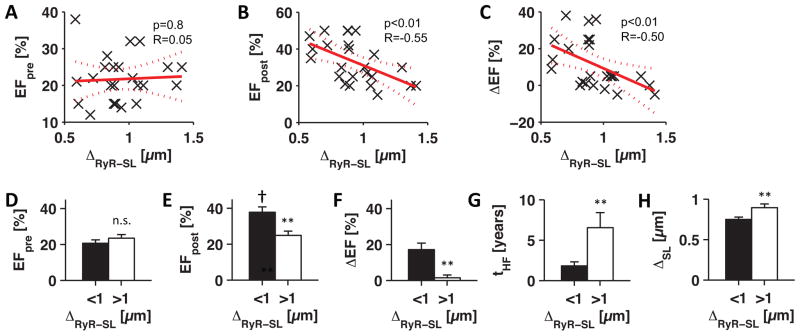
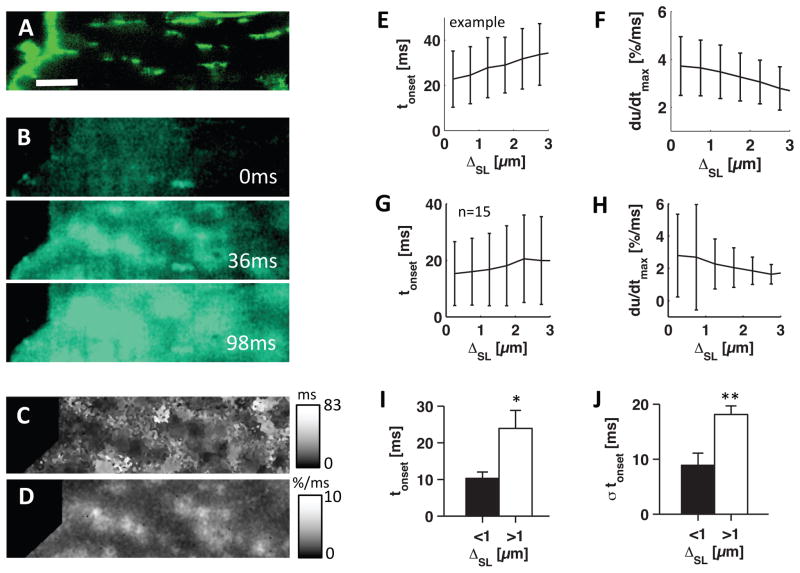
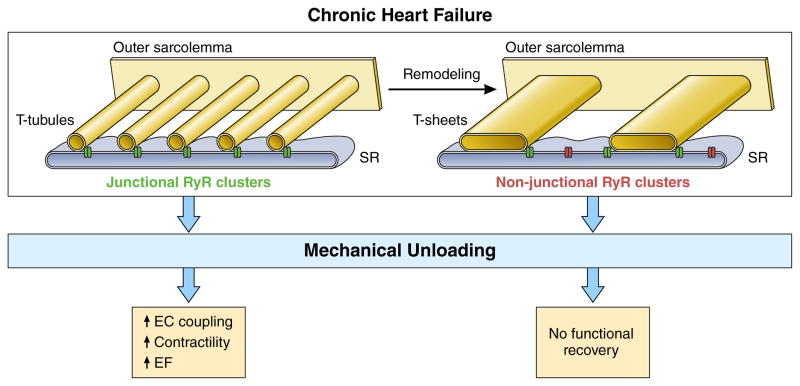
Results: The majority of HF myocytes showed remarkable t-system remodeling, particularly sheet-like invaginations of the sarcolemma. Circularity of t-system components was decreased in HF versus controls (0.37±0.01 versus 0.46±0.02; P<0.01), and the volume/length ratio was increased in HF (0.36±0.01 versus 0.25±0.02 µm2; P<0.0001). T-system density was reduced in HF, leading to increased ryanodine receptor-sarcolemma distances (0.96±0.05 versus 0.64±0.1 µm; P<0.01). Low ryanodine receptor-sarcolemma distances at the time of LVAD implantation predicted high post-LVAD left ventricular ejection fractions (P<0.01) and ejection fraction increases during unloading (P<0.01). Ejection fraction in patients with pre-LVAD ryanodine receptor-sarcolemma distances >1 µm did not improve after mechanical unloading. In addition, calcium transients were recorded in field-stimulated isolated human cardiomyocytes and analyzed with respect to local t-system density. Calcium release in HF myocytes was restricted to regions proximal to the sarcolemma. Local calcium upstroke was delayed (23.9±4.9 versus 10.3±1.7 milliseconds; P<0.05) and more asynchronous (18.1±1.5 versus 8.9±2.2 milliseconds; P<0.01) in HF cells with low t-system density versus cells with high t-system density.
Conclusions: The t-system in end-stage human HF presents a characteristic novel phenotype consisting of sheet-like invaginations of the sarcolemma. Our results suggest that the remodeled t-system impairs excitation-contraction coupling and functional recovery during chronic LVAD unloading. An intact t-system at the time of LVAD implantation may constitute a precondition and predictor for functional cardiac recovery after mechanical unloading.
Keywords: excitation contraction coupling; heart failure; myocytes, cardiac; recovery of function; ryanodine receptor calcium release channels.
© 2017 American Heart Association, Inc.
Figures
Comment in
-
Subcellular Remodeling of the T-Tubule Membrane System: The Limits of Myocardial Recovery Revealed?Circulation. 2017 Apr 25;135(17):1646-1650. doi: 10.1161/CIRCULATIONAHA.117.025319. Circulation. 2017. PMID: 28438805 No abstract available.
Similar articles
-
Subcellular structures and function of myocytes impaired during heart failure are restored by cardiac resynchronization therapy.Circ Res. 2012 Feb 17;110(4):588-97. doi: 10.1161/CIRCRESAHA.111.257428. Epub 2012 Jan 17. Circ Res. 2012. PMID: 22253411 Free PMC article.
-
Myocardial atrophy and chronic mechanical unloading of the failing human heart: implications for cardiac assist device-induced myocardial recovery.J Am Coll Cardiol. 2014 Oct 14;64(15):1602-12. doi: 10.1016/j.jacc.2014.05.073. J Am Coll Cardiol. 2014. PMID: 25301465
-
Mechanical unloading reverses transverse tubule remodelling and normalizes local Ca(2+)-induced Ca(2+)release in a rodent model of heart failure.Eur J Heart Fail. 2012 Jun;14(6):571-80. doi: 10.1093/eurjhf/hfs038. Epub 2012 Apr 1. Eur J Heart Fail. 2012. PMID: 22467752 Free PMC article.
-
Exploring Changes in Myocyte Structure, Contractility, and Energetics From Mechanical Unloading in Patients With Heart Failure Undergoing Ventricular Assist Device Implantation: A Systematic Review and Meta-Analysis.Heart Lung Circ. 2024 Aug;33(8):1097-1116. doi: 10.1016/j.hlc.2024.01.039. Epub 2024 May 4. Heart Lung Circ. 2024. PMID: 38704332 Review.
-
The transverse-axial tubular system of cardiomyocytes.Cell Mol Life Sci. 2013 Dec;70(24):4695-710. doi: 10.1007/s00018-013-1410-5. Epub 2013 Jul 12. Cell Mol Life Sci. 2013. PMID: 23846763 Free PMC article. Review.
Cited by
-
Novel Targets for a Combination of Mechanical Unloading with Pharmacotherapy in Advanced Heart Failure.Int J Mol Sci. 2022 Aug 31;23(17):9886. doi: 10.3390/ijms23179886. Int J Mol Sci. 2022. PMID: 36077285 Free PMC article. Review.
-
Fibrosis and impaired Ca2+ signalling in heart failure.Biophys Rev. 2021 Nov 20;14(1):327-328. doi: 10.1007/s12551-021-00909-3. eCollection 2022 Feb. Biophys Rev. 2021. PMID: 35340608 Free PMC article.
-
Nanoscale regulation of L-type calcium channels differentiates between ischemic and dilated cardiomyopathies.EBioMedicine. 2020 Jul;57:102845. doi: 10.1016/j.ebiom.2020.102845. Epub 2020 Jun 21. EBioMedicine. 2020. PMID: 32580140 Free PMC article.
-
Successful conservative management of left ventricular assist device candidates.ESC Heart Fail. 2023 Feb;10(1):601-615. doi: 10.1002/ehf2.14223. Epub 2022 Nov 15. ESC Heart Fail. 2023. PMID: 36380721 Free PMC article.
-
Quantitative 3D electron microscopy characterization of mitochondrial structure, mitophagy, and organelle interactions in murine atrial fibrillation.J Struct Biol. 2024 Sep;216(3):108110. doi: 10.1016/j.jsb.2024.108110. Epub 2024 Jul 14. J Struct Biol. 2024. PMID: 39009246
References
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Despres JP, Fullerton HJ, Howard VJ, Huffman MD, Isasi CR, Jimenez MC, Judd SE, Kissela BM, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Magid DJ, McGuire DK, Mohler ER, 3rd, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Rosamond W, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Woo D, Yeh RW, Turner MB American Heart Association Statistics C, Stroke Statistics S. Executive Summary: Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation. 2016;133:447–454. - PubMed
-
- Drakos SG, Terrovitis JV, Anastasiou-Nana MI, Nanas JN. Reverse remodeling during long-term mechanical unloading of the left ventricle. J Mol Cell Cardiol. 2007;43:231–42. - PubMed
-
- Birks EJ, George RS, Hedger M, Bahrami T, Wilton P, Bowles CT, Webb C, Bougard R, Amrani M, Yacoub MH, Dreyfus G, Khaghani A. Reversal of severe heart failure with a continuous-flow left ventricular assist device and pharmacological therapy: a prospective study. Circulation. 2011;123:381–390. - PubMed
-
- Birks EJ, Tansley PD, Hardy J, George RS, Bowles CT, Burke M, Banner NR, Khaghani A, Yacoub MH. Left ventricular assist device and drug therapy for the reversal of heart failure. N Engl J Med. 2006;355:1873–1884. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
