

Targeting the energy guardian AMPK: another avenue for treating cardiomyopathy?
- PMID: 27815596
- PMCID: PMC11107559
- DOI: 10.1007/s00018-016-2407-7
Targeting the energy guardian AMPK: another avenue for treating cardiomyopathy?
Abstract
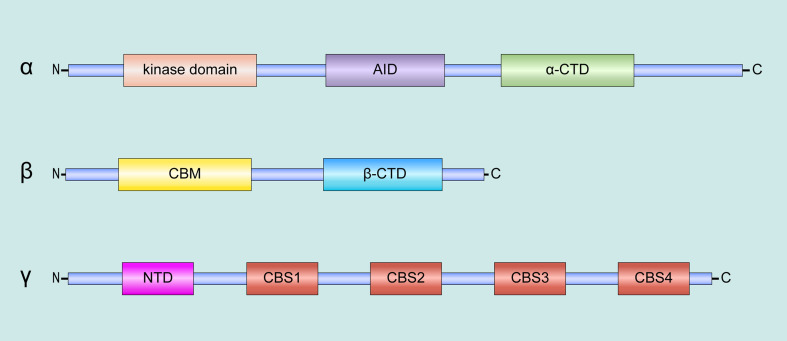
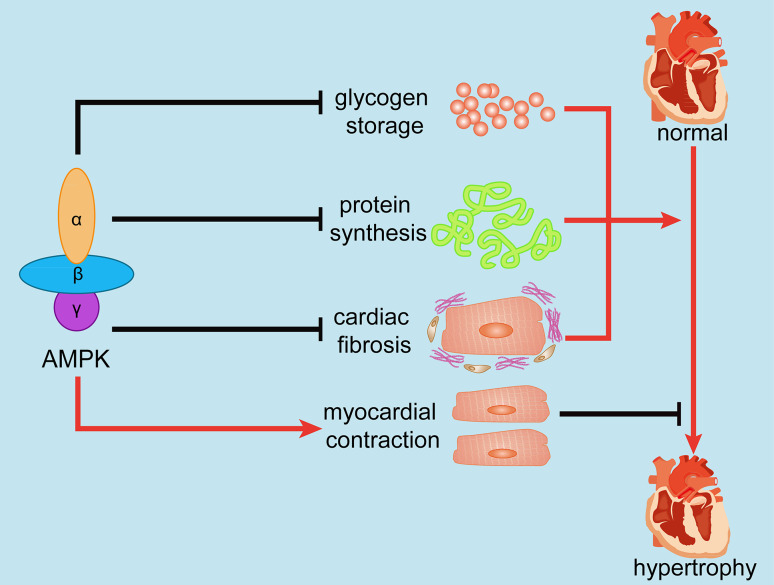
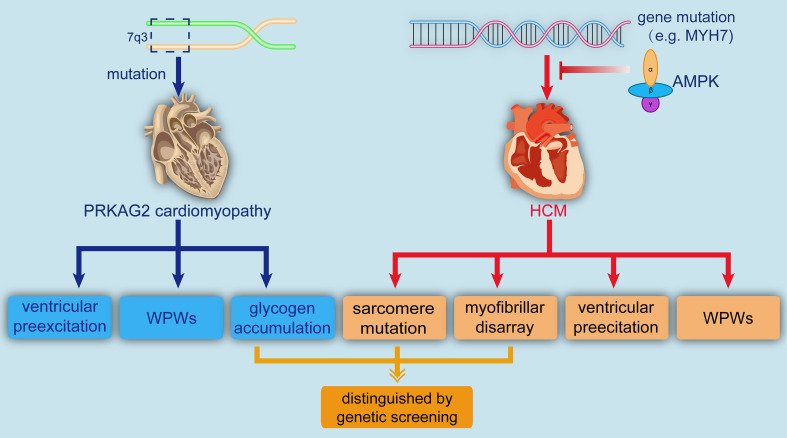
5'-AMP-activated protein kinase (AMPK) is a pivotal regulator of endogenous defensive molecules in various pathological processes. The AMPK signaling regulates a variety of intracellular intermedial molecules involved in biological reactions, including glycogen metabolism, protein synthesis, and cardiac fibrosis, in response to hypertrophic stimuli. Studies have revealed that the activation of AMPK performs a protective role in cardiovascular diseases, whereas its function in cardiac hypertrophy and cardiomyopathy remains elusive and poorly understood. In view of the current evidence of AMPK, we introduce the biological information of AMPK and cardiac hypertrophy as well as some upstream activators of AMPK. Next, we discuss two important types of cardiomyopathy involving AMPK, RKAG2 cardiomyopathy, and hypertrophic cardiomyopathy. Eventually, therapeutic research, genetic screening, conflicts, obstacles, challenges, and potential directions are also highlighted in this review, aimed at providing a comprehensive understanding of AMPK for readers.
Keywords: AMP; Cardiomyocyte; Glycogen storage; Metformin.
Conflict of interest statement
None.
Figures

Similar articles
-
Berberine treatment prevents cardiac dysfunction and remodeling through activation of 5'-adenosine monophosphate-activated protein kinase in type 2 diabetic rats and in palmitate-induced hypertrophic H9c2 cells.Eur J Pharmacol. 2015 Dec 15;769:55-63. doi: 10.1016/j.ejphar.2015.10.043. Epub 2015 Oct 30. Eur J Pharmacol. 2015. PMID: 26522928
-
Improvement of cardiac functions by chronic metformin treatment is associated with enhanced cardiac autophagy in diabetic OVE26 mice.Diabetes. 2011 Jun;60(6):1770-8. doi: 10.2337/db10-0351. Epub 2011 May 11. Diabetes. 2011. PMID: 21562078 Free PMC article.
-
SIRT2 Acts as a Cardioprotective Deacetylase in Pathological Cardiac Hypertrophy.Circulation. 2017 Nov 21;136(21):2051-2067. doi: 10.1161/CIRCULATIONAHA.117.028728. Epub 2017 Sep 25. Circulation. 2017. PMID: 28947430 Free PMC article.
-
AMPK and cardiac remodelling.Sci China Life Sci. 2018 Jan;61(1):14-23. doi: 10.1007/s11427-017-9197-5. Epub 2017 Nov 21. Sci China Life Sci. 2018. PMID: 29170891 Review.
-
AMPK in cardiac fibrosis and repair: Actions beyond metabolic regulation.J Mol Cell Cardiol. 2016 Feb;91:188-200. doi: 10.1016/j.yjmcc.2016.01.001. Epub 2016 Jan 7. J Mol Cell Cardiol. 2016. PMID: 26772531 Review.
Cited by
-
DHHC17 Is a New Regulator of AMPK Signaling.Mol Cell Biol. 2022 Aug 18;42(8):e0013122. doi: 10.1128/mcb.00131-22. Epub 2022 Aug 1. Mol Cell Biol. 2022. PMID: 35913156 Free PMC article.
-
Association of metformin monotherapy or combined therapy with cardiovascular risks in patients with type 2 diabetes mellitus.Cardiovasc Diabetol. 2021 Jan 30;20(1):30. doi: 10.1186/s12933-020-01202-5. Cardiovasc Diabetol. 2021. PMID: 33516224 Free PMC article.
-
AMPK: a balancer of the renin-angiotensin system.Biosci Rep. 2019 Sep 3;39(9):BSR20181994. doi: 10.1042/BSR20181994. Print 2019 Sep 30. Biosci Rep. 2019. PMID: 31413168 Free PMC article. Review.
-
Novel roles of κ-opioid receptor in myocardial ischemia-reperfusion injury.PeerJ. 2024 Jun 25;12:e17333. doi: 10.7717/peerj.17333. eCollection 2024. PeerJ. 2024. PMID: 38948204 Free PMC article. Review.
-
RUNX3 Inhibits the Invasion and Metastasis of Human Colon Cancer HT-29 Cells by Upregulating MMP-2/9.Evid Based Complement Alternat Med. 2020 Feb 27;2020:5978131. doi: 10.1155/2020/5978131. eCollection 2020. Evid Based Complement Alternat Med. 2020. PMID: 32184893 Free PMC article.
References
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Despres JP, Fullerton HJ, Howard VJ, Huffman MD, Isasi CR, Jimenez MC, Judd SE, Kissela BM, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Magid DJ, McGuire DK, Mohler ER 3rd, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Rosamond W, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Woo D, Yeh RW, Turner MB; American Heart Association Statistics C, Stroke Statistics S (2016) Heart disease and stroke statistics-2016 update: a report from the American Heart Association. Circulation 133:e38–e360 - PubMed
-
- Maron BJ, Towbin JA, Thiene G, Antzelevitch C, Corrado D, Arnett D, Moss AJ, Seidman CE, Young JB, American Heart A, Council on Clinical Cardiology HF, Transplantation C, Quality of C, Outcomes R, Functional G, Translational Biology Interdisciplinary Working G, Council on E, Prevention (2006) Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation 113:1807–1816 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
