

The immune system's role in sepsis progression, resolution, and long-term outcome
- PMID: 27782333
- PMCID: PMC5111634
- DOI: 10.1111/imr.12499
The immune system's role in sepsis progression, resolution, and long-term outcome
Abstract
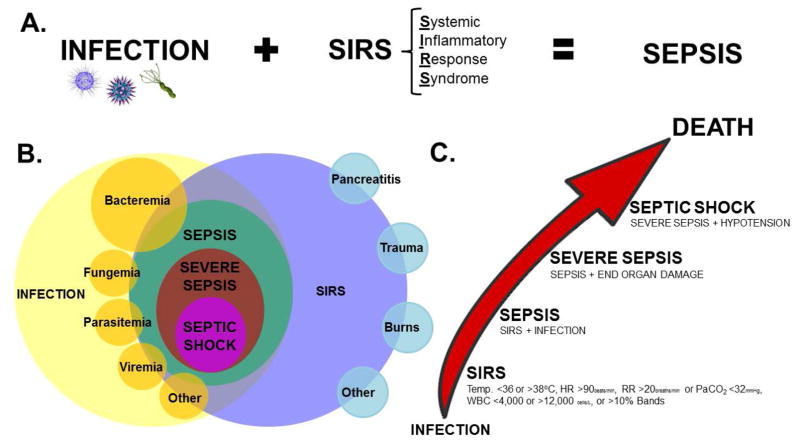
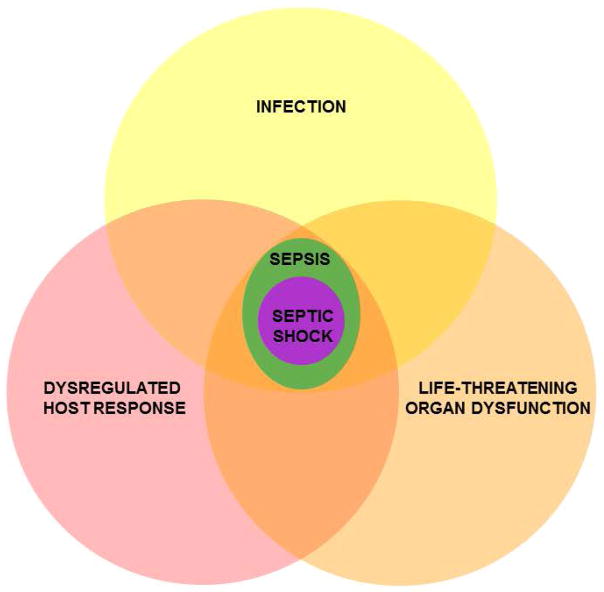
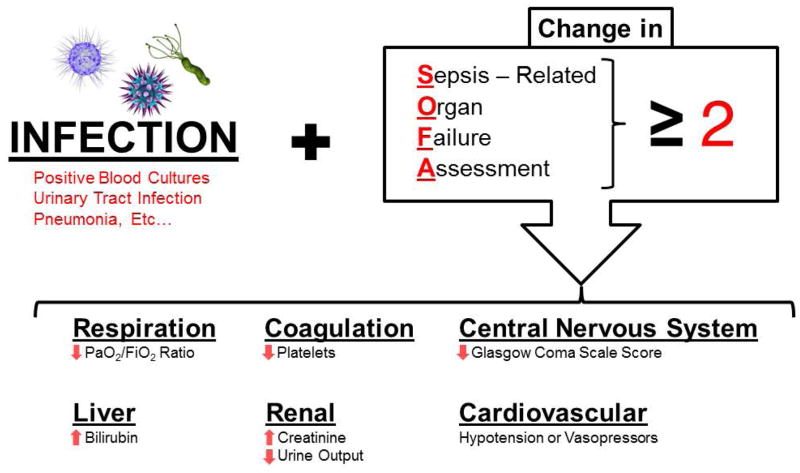
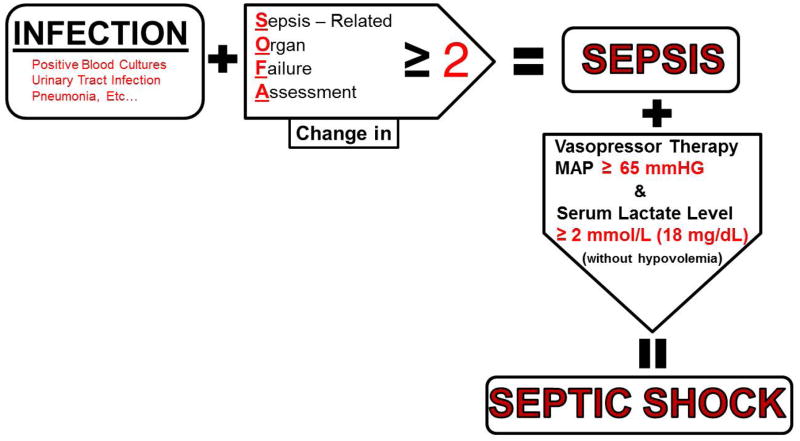
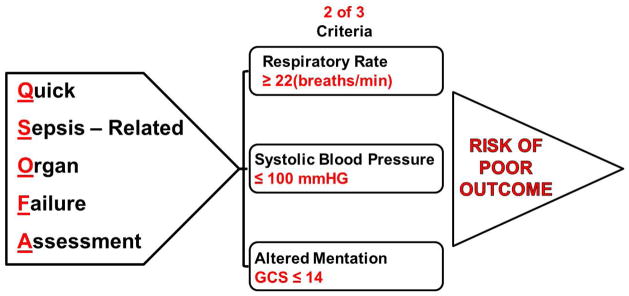
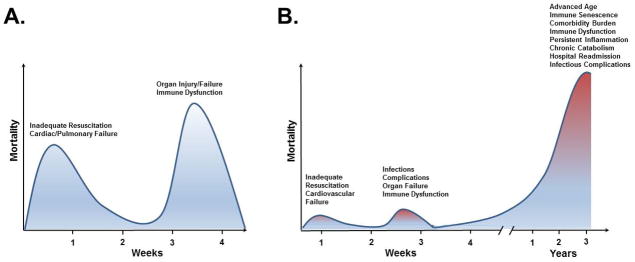
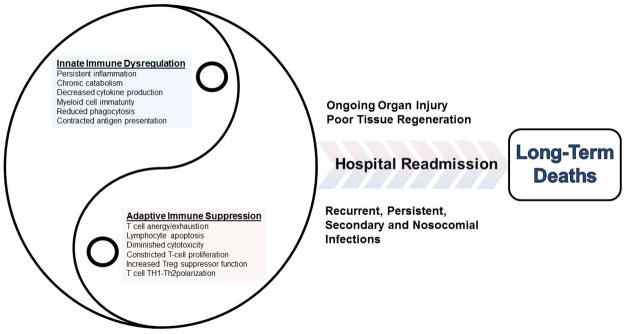
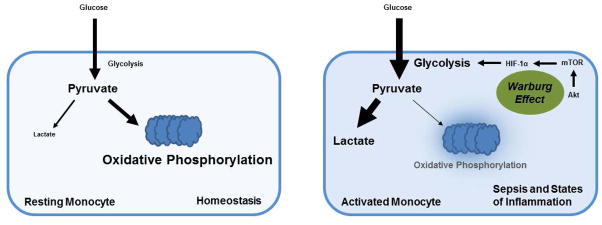
Sepsis occurs when an infection exceeds local tissue containment and induces a series of dysregulated physiologic responses that result in organ dysfunction. A subset of patients with sepsis progress to septic shock, defined by profound circulatory, cellular, and metabolic abnormalities, and associated with a greater mortality. Historically, sepsis-induced organ dysfunction and lethality were attributed to the complex interplay between the initial inflammatory and later anti-inflammatory responses. With advances in intensive care medicine and goal-directed interventions, early 30-day sepsis mortality has diminished, only to steadily escalate long after "recovery" from acute events. As so many sepsis survivors succumb later to persistent, recurrent, nosocomial, and secondary infections, many investigators have turned their attention to the long-term sepsis-induced alterations in cellular immune function. Sepsis clearly alters the innate and adaptive immune responses for sustained periods of time after clinical recovery, with immune suppression, chronic inflammation, and persistence of bacterial representing such alterations. Understanding that sepsis-associated immune cell defects correlate with long-term mortality, more investigations have centered on the potential for immune modulatory therapy to improve long-term patient outcomes. These efforts are focused on more clearly defining and effectively reversing the persistent immune cell dysfunction associated with long-term sepsis mortality.
Keywords: adaptive immune dysfunction; immune suppression sepsis; inflammation; innate immune dysfunction; sepsis.
© 2016 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare there are no commercial or financial conflicts of interest related to the studies.
Figures
Similar articles
-
Sepsis-induced immune dysfunction: can immune therapies reduce mortality?J Clin Invest. 2016 Jan;126(1):23-31. doi: 10.1172/JCI82224. Epub 2016 Jan 4. J Clin Invest. 2016. PMID: 26727230 Free PMC article. Review.
-
Diabetes and Sepsis: Risk, Recurrence, and Ruination.Front Endocrinol (Lausanne). 2017 Oct 30;8:271. doi: 10.3389/fendo.2017.00271. eCollection 2017. Front Endocrinol (Lausanne). 2017. PMID: 29163354 Free PMC article. Review.
-
Innate Immunity in the Persistent Inflammation, Immunosuppression, and Catabolism Syndrome and Its Implications for Therapy.Front Immunol. 2018 Apr 4;9:595. doi: 10.3389/fimmu.2018.00595. eCollection 2018. Front Immunol. 2018. PMID: 29670613 Free PMC article. Review.
-
Role of cellular events in the pathophysiology of sepsis.Inflamm Res. 2016 Nov;65(11):853-868. doi: 10.1007/s00011-016-0970-x. Epub 2016 Jul 8. Inflamm Res. 2016. PMID: 27392441 Review.
-
Management of Sepsis-Induced Immunosuppression.Crit Care Clin. 2018 Jan;34(1):97-106. doi: 10.1016/j.ccc.2017.08.007. Epub 2017 Oct 6. Crit Care Clin. 2018. PMID: 29149944 Review.
Cited by
-
A pairwise cytokine code explains the organism-wide response to sepsis.Nat Immunol. 2024 Feb;25(2):226-239. doi: 10.1038/s41590-023-01722-8. Epub 2024 Jan 8. Nat Immunol. 2024. PMID: 38191855 Free PMC article.
-
Medicinal nicotine in COVID-19 acute respiratory distress syndrome, the new corticosteroid.World J Crit Care Med. 2022 Jul 9;11(4):228-235. doi: 10.5492/wjccm.v11.i4.228. eCollection 2022 Jul 9. World J Crit Care Med. 2022. PMID: 36051943 Free PMC article. Review.
-
Attributable Mortality of Hip Fracture in Older Patients: A Retrospective Observational Study.J Clin Med. 2020 Jul 24;9(8):2370. doi: 10.3390/jcm9082370. J Clin Med. 2020. PMID: 32722204 Free PMC article.
-
Role of Zinc in Neonatal Sepsis.Indian J Pediatr. 2021 Jul;88(7):696-702. doi: 10.1007/s12098-021-03748-y. Epub 2021 Apr 24. Indian J Pediatr. 2021. PMID: 33893972 Review.
-
Dynamical modeling of pro- and anti-inflammatory cytokines in the early stage of septic shock.In Silico Biol. 2020;14(1-2):101-121. doi: 10.3233/ISB-200474. In Silico Biol. 2020. PMID: 32597796 Free PMC article.
References
-
- American College of Chest Physicians/Society of Critical Care Medicine Consensus. Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med. 1992;20:864–874. - PubMed
-
- Levy MM, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med. 2003;31:1250–1256. - PubMed
-
- Kaukonen KM, Bailey M, Pilcher D, Cooper DJ, Bellomo R. Systemic inflammatory response syndrome criteria in defining severe sepsis. N Engl J Med. 2015;372:1629–1638. - PubMed
-
- Gaieski DF, Edwards JM, Kallan MJ, Carr BG. Benchmarking the incidence and mortality of severe sepsis in the United States. Crit Care Med. 2013;41:1167–1174. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
