

Association between pretreatment Glasgow prognostic score and gastric cancer survival and clinicopathological features: a meta-analysis
- PMID: 27390529
- PMCID: PMC4930270
- DOI: 10.2147/OTT.S103996
Association between pretreatment Glasgow prognostic score and gastric cancer survival and clinicopathological features: a meta-analysis
Abstract
Background: Glasgow prognostic score (GPS) is widely known as a systemic inflammatory-based marker. The relationship between pretreatment GPS and gastric cancer (GC) survival and clinicopathological features remains controversial. The aim of the study was to conduct a meta-analysis of published studies to evaluate the association between pretreatment GPS and survival and clinicopathological features in GC patients.
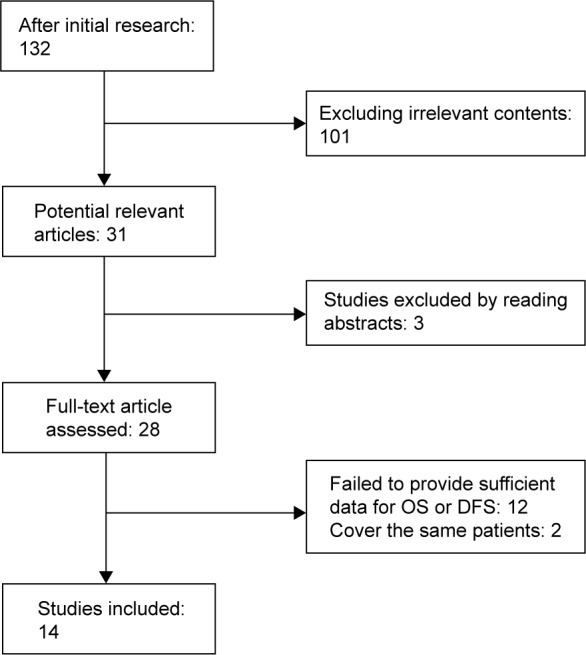
Methods: We searched PubMed, Embase, MEDLINE, and BioMed databases for relevant studies. Combined analyses were used to assess the association between pretreatment GPS and overall survival, disease-free survival, and clinicopathological parameters by Stata Version 12.0.
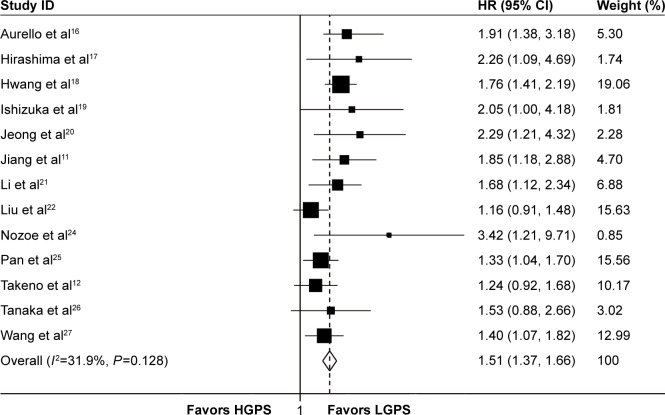
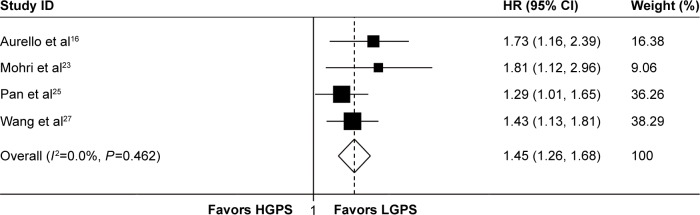
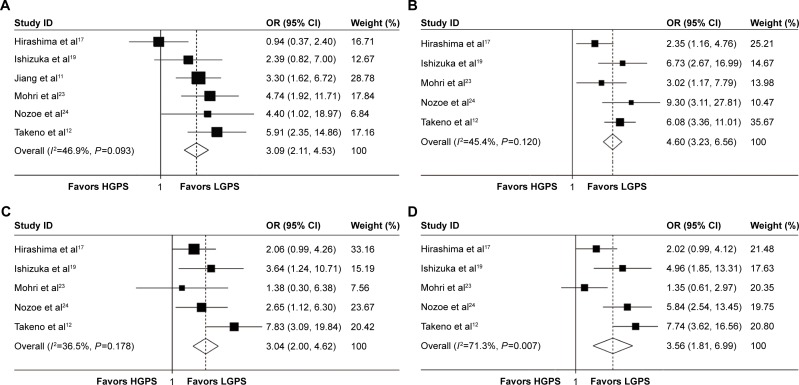
Results: A total of 14 studies were included in this meta-analysis, including 5,579 GC patients. The results indicated that pretreatment high GPS (HGPS) predicted poor overall survival (hazard ratio =1.51, 95% CI: 1.37-1.66, P<0.01) and disease-free survival (hazard ratio =1.45, 95% CI: 1.26-1.68, P<0.01) in GC patients. Pretreatment HGPS was also significantly associated with advanced tumor-node-metastasis stage (odds ratio [OR] =3.09, 95% CI: 2.11-4.53, P<0.01), lymph node metastasis (OR =4.60, 95% CI: 3.23-6.56, P<0.01), lymphatic invasion (OR =3.04, 95% CI: 2.00-4.62, P<0.01), and venous invasion (OR =3.56, 95% CI: 1.81-6.99, P<0.01).
Conclusion: Our meta-analysis indicated that pretreatment HGPS could be a predicative factor of poor survival outcome and clinicopathological features for GC patients.
Keywords: Glasgow prognostic score; clinicopathological feature; gastric cancer; survival.
Figures
Similar articles
-
Prognostic Value of Pretreatment Systemic Immune-Inflammation Index in Gastric Cancer: A Meta-Analysis.Front Oncol. 2021 Mar 11;11:537140. doi: 10.3389/fonc.2021.537140. eCollection 2021. Front Oncol. 2021. PMID: 33777726 Free PMC article.
-
Prognostic Value of Pretreatment Glasgow Prognostic Score/Modified Glasgow Prognostic Score in Ovarian Cancer: A Systematic Review and Meta-Analysis.Nutr Cancer. 2022;74(6):1968-1975. doi: 10.1080/01635581.2021.1980591. Epub 2021 Sep 22. Nutr Cancer. 2022. PMID: 34549675
-
Clinicopathological and prognostic significance of pretreatment thrombocytosis in patients with endometrial cancer: a meta-analysis.Cancer Manag Res. 2019 May 8;11:4283-4295. doi: 10.2147/CMAR.S186535. eCollection 2019. Cancer Manag Res. 2019. PMID: 31190994 Free PMC article.
-
Clinical and prognostic significances of cancer stem cell markers in gastric cancer patients: a systematic review and meta-analysis.Cancer Cell Int. 2021 Feb 27;21(1):139. doi: 10.1186/s12935-021-01840-z. Cancer Cell Int. 2021. PMID: 33639931 Free PMC article. Review.
-
Prognostic and clinicopathological value of the geriatric nutritional risk index in gastric cancer: A meta-analysis of 5,834 patients.Front Surg. 2023 Jan 6;9:1087298. doi: 10.3389/fsurg.2022.1087298. eCollection 2022. Front Surg. 2023. PMID: 36684163 Free PMC article. Review.
Cited by
-
Combined fibrinogen and neutrophil-lymphocyte ratio as a predictive factor in resectable colorectal adenocarcinoma.Cancer Manag Res. 2018 Nov 26;10:6285-6294. doi: 10.2147/CMAR.S161094. eCollection 2018. Cancer Manag Res. 2018. PMID: 30568490 Free PMC article.
-
Angiogenesis and inflammation at the crossroads between diabetes and cancer: PS226.Porto Biomed J. 2017 Sep-Oct;2(5):227-228. doi: 10.1016/j.pbj.2017.07.120. Epub 2017 Sep 1. Porto Biomed J. 2017. PMID: 32258731 Free PMC article. No abstract available.
-
CD147 overexpression may serve as a promising diagnostic and prognostic marker for gastric cancer: evidence from original research and literature.Oncotarget. 2017 May 9;8(19):30888-30899. doi: 10.18632/oncotarget.15737. Oncotarget. 2017. PMID: 28427166 Free PMC article.
-
Prognostic nutritional index as a prognostic biomarker for survival in digestive system carcinomas.Oncotarget. 2016 Dec 27;7(52):86573-86583. doi: 10.18632/oncotarget.13472. Oncotarget. 2016. PMID: 27888808 Free PMC article.
-
The Prognostic Role of Glasgow Prognostic Score and C-reactive Protein to Albumin Ratio for Sarcoma: A System Review and Meta-Analysis.Dis Markers. 2020 Jan 7;2020:8736509. doi: 10.1155/2020/8736509. eCollection 2020. Dis Markers. 2020. PMID: 31998420 Free PMC article.
References
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. Ca-Cancer J Clin. 2015;65(2):87–108. - PubMed
-
- Peng CW, Wang LW, Zeng WJ, Yang XJ, Li Y. Evaluation of the staging systems for gastric cancer. J Surg Oncol. 2013;108(2):93–105. - PubMed
-
- MacDonald N. Cancer cachexia and targeting chronic inflammation: a unified approach to cancer treatment and palliative/supportive care. J Support Oncol. 2007;5(4):157–162. discussion 164–156, 183. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
