

Age, Spatial, and Temporal Variations in Hospital Admissions with Malaria in Kilifi County, Kenya: A 25-Year Longitudinal Observational Study
- PMID: 27352303
- PMCID: PMC4924798
- DOI: 10.1371/journal.pmed.1002047
Age, Spatial, and Temporal Variations in Hospital Admissions with Malaria in Kilifi County, Kenya: A 25-Year Longitudinal Observational Study
Abstract
Background: Encouraging progress has been seen with reductions in Plasmodium falciparum malaria transmission in some parts of Africa. Reduced transmission might lead to increasing susceptibility to malaria among older children due to lower acquired immunity, and this has implications for ongoing control strategies.
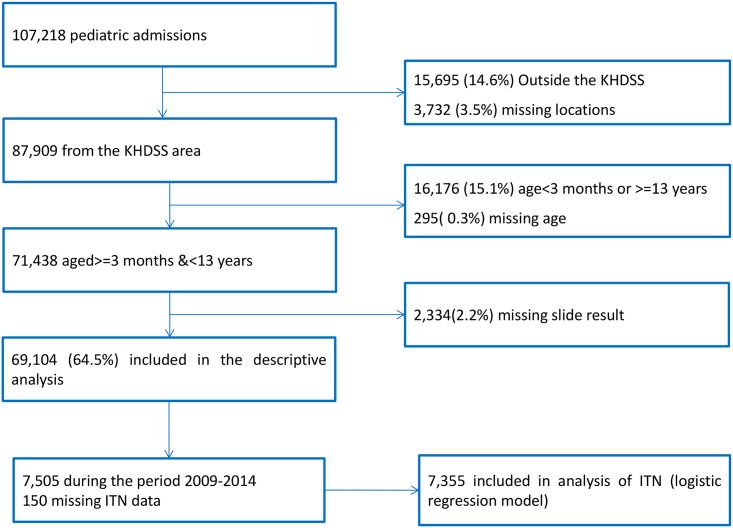
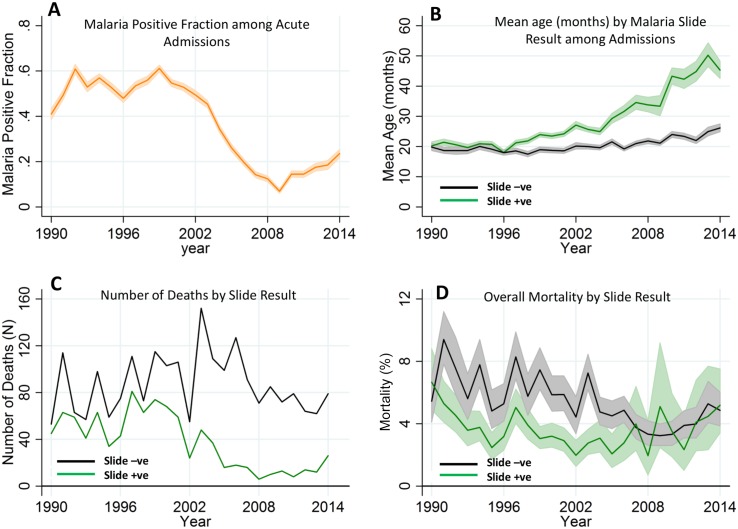
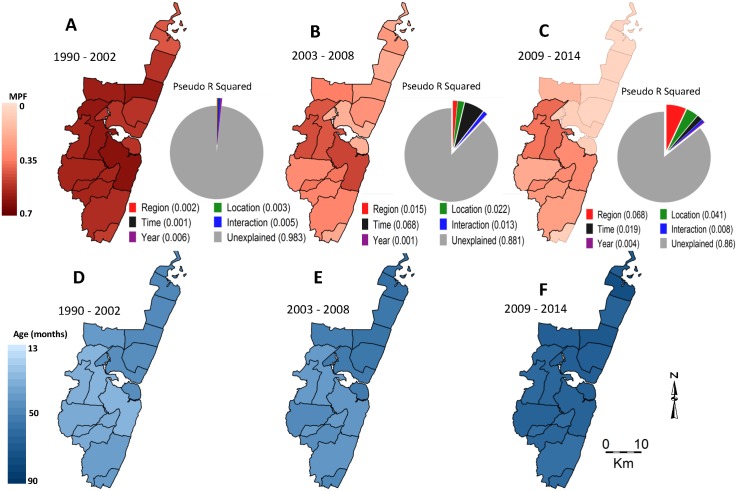
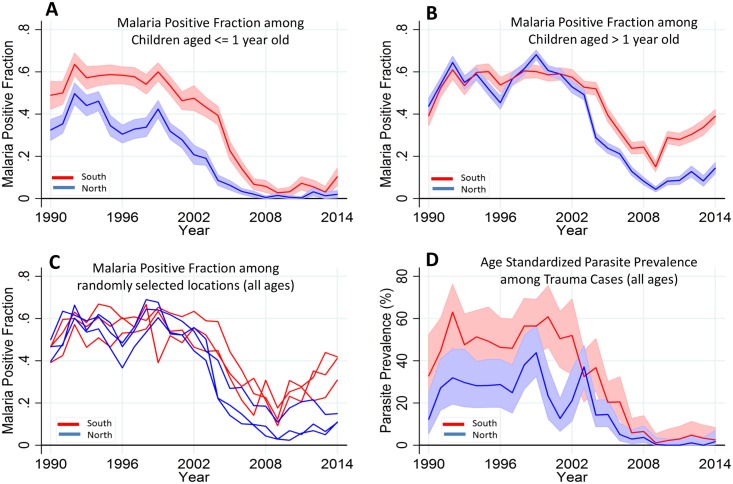
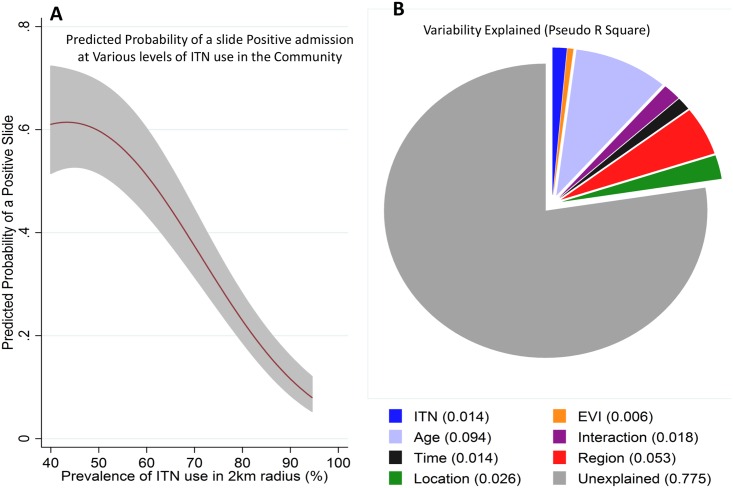
Methods and findings: We conducted a longitudinal observational study of children admitted to Kilifi County Hospital in Kenya and linked it to data on residence and insecticide-treated net (ITN) use. This included data from 69,104 children aged from 3 mo to 13 y admitted to Kilifi County Hospital between 1 January 1990 and 31 December 2014. The variation in malaria slide positivity among admissions was examined in logistic regression models using the following predictors: location of the residence, calendar time, the child's age, ITN use, and the enhanced vegetation index (a proxy for soil moisture). The proportion of malaria slide-positive admissions declined from 0.56 (95% confidence interval [CI] 0.54-0.58) in 1998 to 0.07 (95% CI 0.06-0.08) in 2009 but then increased again through to 0.24 (95% CI 0.22-0.25) in 2014. Older children accounted for most of the increase after 2009 (0.035 [95% CI 0.030-0.040] among young children compared to 0.22 [95% CI 0.21-0.23] in older children). There was a nonlinear relationship between malaria risk and prevalence of ITN use within a 2 km radius of an admitted child's residence such that the predicted malaria positive fraction varied from ~0.4 to <0.1 as the prevalence of ITN use varied from 20% to 80%. In this observational analysis, we were unable to determine the cause of the decline in malaria between 1998 and 2009, which pre-dated the dramatic scale-up in ITN distribution and use.
Conclusion: Following a period of reduced transmission, a cohort of older children emerged who have increased susceptibility to malaria. Further reductions in malaria transmission are needed to mitigate the increasing burden among older children, and universal ITN coverage is a promising strategy to achieve this goal.
Conflict of interest statement
AN serves on the
Figures
Comment in
-
Malaria Epidemiology in Kilifi, Kenya during the 21st Century: What Next?PLoS Med. 2016 Jun 28;13(6):e1002048. doi: 10.1371/journal.pmed.1002048. eCollection 2016 Jun. PLoS Med. 2016. PMID: 27351181 Free PMC article.
Similar articles
-
Trends in malaria cases, hospital admissions and deaths following scale-up of anti-malarial interventions, 2000-2010, Rwanda.Malar J. 2012 Jul 23;11:236. doi: 10.1186/1475-2875-11-236. Malar J. 2012. PMID: 22823945 Free PMC article.
-
Trends in bednet ownership and usage, and the effect of bednets on malaria hospitalization in the Kilifi Health and Demographic Surveillance System (KHDSS): 2008-2015.BMC Infect Dis. 2017 Nov 15;17(1):720. doi: 10.1186/s12879-017-2822-x. BMC Infect Dis. 2017. PMID: 29141606 Free PMC article.
-
Targeting remaining pockets of malaria transmission in Kenya to hasten progress towards national elimination goals: an assessment of prevalence and risk factors in children from the Lake endemic region.Malar J. 2019 Jul 12;18(1):233. doi: 10.1186/s12936-019-2876-x. Malar J. 2019. PMID: 31299976 Free PMC article.
-
Evaluation of universal coverage of insecticide-treated nets in western Kenya: field surveys.Malar J. 2014 Sep 3;13:351. doi: 10.1186/1475-2875-13-351. Malar J. 2014. PMID: 25187326 Free PMC article.
-
Spatiotemporal analysis of insecticide-treated net use for children under 5 in relation to socioeconomic gradients in Central and East Africa.Malar J. 2020 Apr 22;19(1):163. doi: 10.1186/s12936-020-03236-2. Malar J. 2020. PMID: 32321547 Free PMC article.
Cited by
-
Malaria attributable fractions with changing transmission intensity: Bayesian latent class vs logistic models.Malar J. 2022 Nov 11;21(1):326. doi: 10.1186/s12936-022-04346-9. Malar J. 2022. PMID: 36369045 Free PMC article.
-
A cross-sectional analysis identifies a low prevalence of Plasmodium ovale species infections in symptomatic and asymptomatic individuals in Kilifi county, Kenya.Wellcome Open Res. 2024 Sep 17;7:207. doi: 10.12688/wellcomeopenres.17972.4. eCollection 2022. Wellcome Open Res. 2024. PMID: 39364258 Free PMC article.
-
Plasmodium falciparum adapts its investment into replication versus transmission according to the host environment.Elife. 2023 Mar 14;12:e85140. doi: 10.7554/eLife.85140. Elife. 2023. PMID: 36916164 Free PMC article.
-
Impact of Intermittent Presumptive Treatment for Malaria in Pregnancy on Hospital Birth Outcomes on the Kenyan Coast.Clin Infect Dis. 2023 Feb 8;76(3):e875-e883. doi: 10.1093/cid/ciac509. Clin Infect Dis. 2023. PMID: 35731850 Free PMC article.
-
Trend of Malaria Burden Among Residents of Kisii County, Kenya After More Than a Decade Usage of Artemisinin Combined Therapies, 11-Year Laboratory Based Retrospective Study.Infect Drug Resist. 2022 Sep 6;15:5221-5232. doi: 10.2147/IDR.S370218. eCollection 2022. Infect Drug Resist. 2022. PMID: 36097528 Free PMC article.
References
-
- Noor AM, Kinyoki DK, Mundia CW, Kabaria CW, Mutua JW, Alegana VA, et al. The changing risk of Plasmodium falciparum malaria infection in Africa: 2000–10: a spatial and temporal analysis of transmission intensity. Lancet. 2014;383(9930):1739–47. Epub 2014/02/25. 10.1016/s0140-6736(13)62566-0 ; PubMed Central PMCID: PMCPmc4030588. - DOI - PMC - PubMed
-
- Woolhouse ME. Patterns in parasite epidemiology: the peak shift. Parasitol Today. 1998;14(10):428–34. Epub 2006/10/17. . - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
