

Frequent occurrence of therapeutically reversible CMV-associated encephalopathy during radiotherapy of the brain
- PMID: 27286796
- PMCID: PMC5793811
- DOI: 10.1093/neuonc/now120
Frequent occurrence of therapeutically reversible CMV-associated encephalopathy during radiotherapy of the brain
Abstract
Background: Neurological decline during radio(chemo)therapy of the brain is often attributed to disease progression or side effects of radiotherapy. Diagnosis of opportunistic neurotropic infections such as cytomegalovirus (CMV) infections is uncommon, even though high-grade gliomas and some brain metastases are known to contain CMV particles. We prospectively examined the frequency of CMV encephalopathy during radiotherapy of the brain.
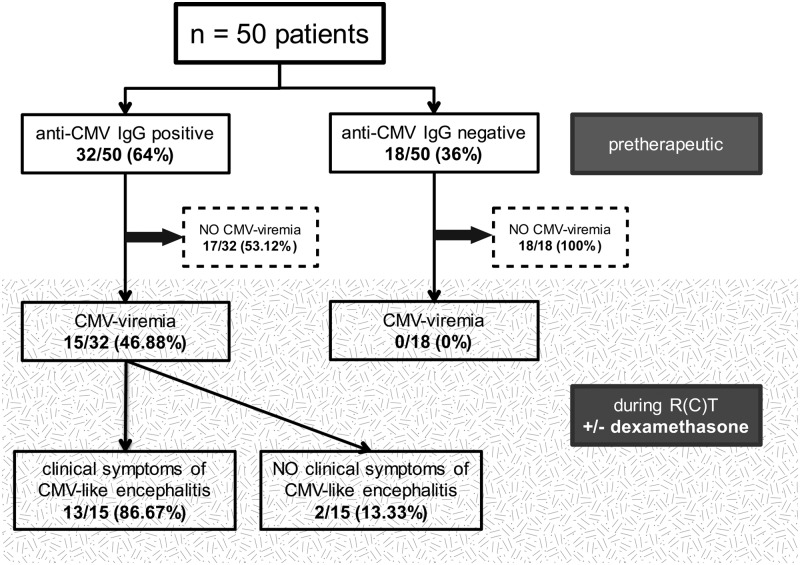
Methods: Fifty patients requiring whole-brain radiotherapy for brain metastases (n = 27) or local radio(chemo)therapy of the brain for high-grade gliomas (n = 23) were observed in the prospective observational GLIO-CMV-01 study. MRIs and blood samples were obtained before, halfway through, and at the end of radiotherapy. MRIs were screened for disease progression or increased intracranial pressure. Blood was tested for anti-CMV immunoglobulin (Ig)M, anti-CMV IgG, and CMV DNA.
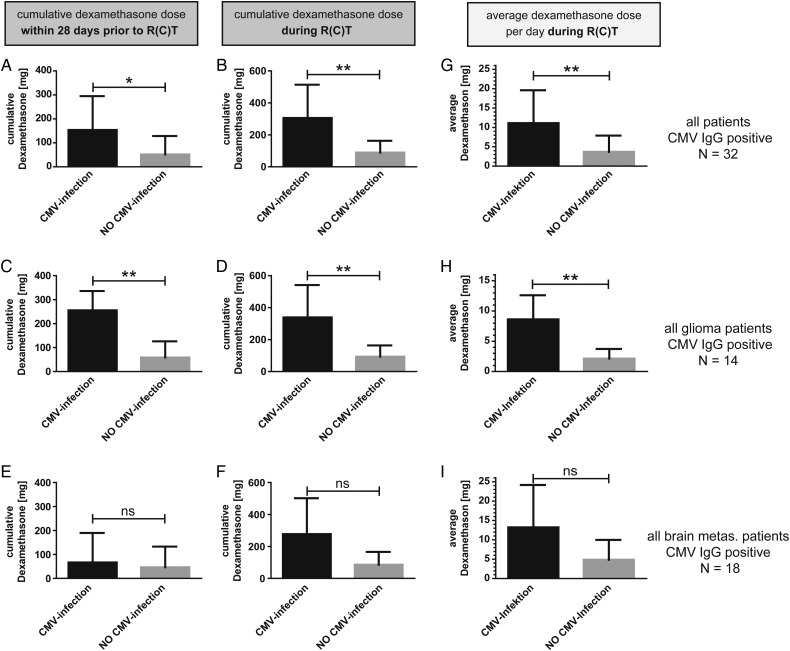
Results: Thirty-two of 50 (64%) patients were positive for anti-CMV IgG before radio(chemo)therapy. Fifteen of those 32 (48%) developed viremia during or up to 28 days after treatment. Thirteen of those 15 (87%) required treatment for CMV-associated encephalopathy. MRIs were negative for disease progression, edema, or bleeding. None of the patients negative for anti-CMV IgG developed viremia, suggesting a reactivation rather than a primary infection.In the group at risk consisting of anti-CMV IgG+ patients, age >65 (P = .004) and the amount of dexamethasone taken during radio(chemo)therapy (P = .004) were associated with an increased risk for CMV-associated encephalopathy. One hundred and fifty days after the start of radio(chemo)therapy, survival was 74% (14/19) (no encephalopathy) versus 54% (7/13) (encephalopathy) (odds ratio, 0.42; 95% CI, 0.03-1.86; P = .25).
Conclusion: CMV reactivation frequently causes encephalopathy during radio(chemo)therapy of the brain. The unexpected high incidence of this infection makes it highly clinically relevant for every treating physician.
Keywords: brain metastases; cytomegalovirus; glioblastoma; infection; radiotherapy.
© The Author(s) 2016. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures

Similar articles
-
Cytomegalovirus and Glioblastoma: A Review of the Biological Associations and Therapeutic Strategies.J Clin Med. 2022 Sep 4;11(17):5221. doi: 10.3390/jcm11175221. J Clin Med. 2022. PMID: 36079151 Free PMC article. Review.
-
Clinically significant CMV (re)activation during or after radiotherapy/chemotherapy of the brain : Correlation with neurological deterioration and improvement upon antiviral treatment.Strahlenther Onkol. 2016 Jul;192(7):489-97. doi: 10.1007/s00066-016-0987-7. Epub 2016 May 31. Strahlenther Onkol. 2016. PMID: 27245820 English.
-
Prospective Evaluation of CD45RA+/CCR7- Effector Memory T (TEMRA) Cell Subsets in Patients with Primary and Secondary Brain Tumors during Radiotherapy of the Brain within the Scope of the Prospective Glio-CMV-01 Clinical Trial.Cells. 2023 Feb 4;12(4):516. doi: 10.3390/cells12040516. Cells. 2023. PMID: 36831183 Free PMC article.
-
Predictive factors of human cytomegalovirus reactivation in newly diagnosed glioblastoma patients treated with chemoradiotherapy.J Neurovirol. 2021 Feb;27(1):94-100. doi: 10.1007/s13365-020-00922-4. Epub 2021 Jan 6. J Neurovirol. 2021. PMID: 33405205
-
Cytomegalovirus in human brain tumors: Role in pathogenesis and potential treatment options.World J Exp Med. 2015 Feb 20;5(1):1-10. doi: 10.5493/wjem.v5.i1.1. eCollection 2015 Feb 20. World J Exp Med. 2015. PMID: 25699229 Free PMC article. Review.
Cited by
-
Human cytomegalovirus seropositivity is associated with decreased survival in glioblastoma patients.Neurooncol Adv. 2019 Sep 7;1(1):vdz020. doi: 10.1093/noajnl/vdz020. eCollection 2019 May-Dec. Neurooncol Adv. 2019. PMID: 32642656 Free PMC article.
-
Profiling of microRNAs modulating cytomegalovirus infection in astrocytoma patients.Neurol Sci. 2018 Nov;39(11):1895-1902. doi: 10.1007/s10072-018-3518-8. Epub 2018 Aug 8. Neurol Sci. 2018. PMID: 30090984
-
Human cytomegalovirus and Epstein-Barr virus infections increase the risk of death in patients with head and neck cancers receiving radiotherapy or radiochemotherapy.Medicine (Baltimore). 2018 Dec;97(51):e13777. doi: 10.1097/MD.0000000000013777. Medicine (Baltimore). 2018. PMID: 30572533 Free PMC article.
-
Cytomegalovirus and Glioblastoma: A Review of the Biological Associations and Therapeutic Strategies.J Clin Med. 2022 Sep 4;11(17):5221. doi: 10.3390/jcm11175221. J Clin Med. 2022. PMID: 36079151 Free PMC article. Review.
-
Cytomegalovirus Seropositivity and Suicidal Behavior: A Mini-Review.Medicina (Kaunas). 2019 Dec 12;55(12):782. doi: 10.3390/medicina55120782. Medicina (Kaunas). 2019. PMID: 31842504 Free PMC article.
References
-
- Lewis RM, Johnson PC, Golden D et al. . The adverse impact of cytomegalovirus infection on clinical outcome in cyclosporine-prednisone treated renal allograft recipients. Transplantation. 1988;45(2):353–359. - PubMed
-
- Okita Y, Narita Y, Miyakita Y et al. . Management of cytomegalovirus infection in a patient with malignant glioma treated with temozolomide and steroids. Intern Med. 2012;51(20):2967–2971. - PubMed
-
- Crough T, Beagley L, Smith C et al. . Ex vivo functional analysis, expansion and adoptive transfer of cytomegalovirus-specific T-cells in patients with glioblastoma multiforme. Immunol Cell Biol. 2012;90(9):872–880. - PubMed
-
- Soderberg-Naucler C, Rahbar A, Stragliotto G. Survival in patients with glioblastoma receiving valganciclovir. N Engl J Med. 2013;369(10):985–986. - PubMed
-
- Lehrer S, Green S, Ramanathan L et al. . No consistent relationship of glioblastoma incidence and cytomegalovirus seropositivity in whites, blacks, and Hispanics. Anticancer Res. 2012;32(3):1113–1115. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
