

A Risk Prediction Model Based on Lymph-Node Metastasis in Poorly Differentiated-Type Intramucosal Gastric Cancer
- PMID: 27228258
- PMCID: PMC4881979
- DOI: 10.1371/journal.pone.0156207
A Risk Prediction Model Based on Lymph-Node Metastasis in Poorly Differentiated-Type Intramucosal Gastric Cancer
Abstract
Background and aim: Endoscopic submucosal dissection (ESD) for undifferentiated type early gastric cancer is regarded as an investigational treatment. Few studies have tried to identify the risk factors that predict lymph-node metastasis (LNM) in intramucosal poorly differentiated adenocarcinomas (PDC). This study was designed to develop a risk scoring system (RSS) for predicting LNM in intramucosal PDC.
Methods: From January 2002 to July 2015, patients diagnosed with mucosa-confined PDC, among those who underwent curative gastrectomy with lymph node dissection were reviewed. A risk model based on independent predicting factors of LNM was developed, and its performance was internally validated using a split sample approach.
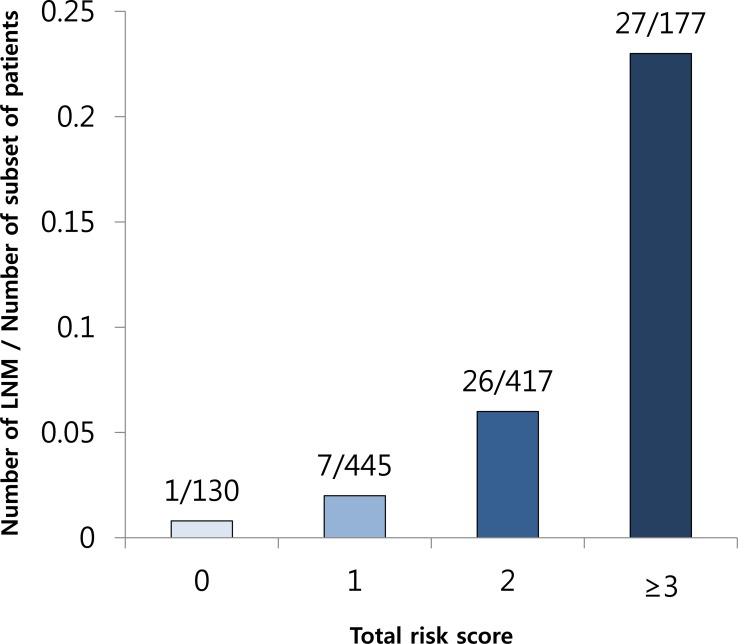
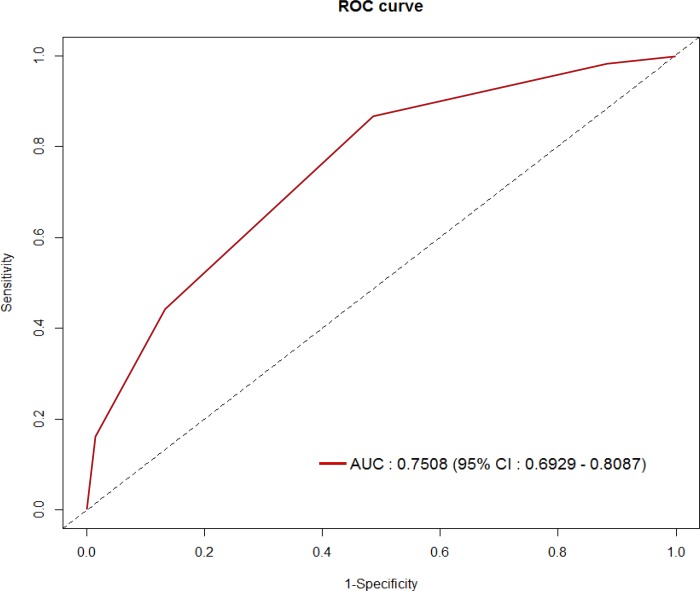
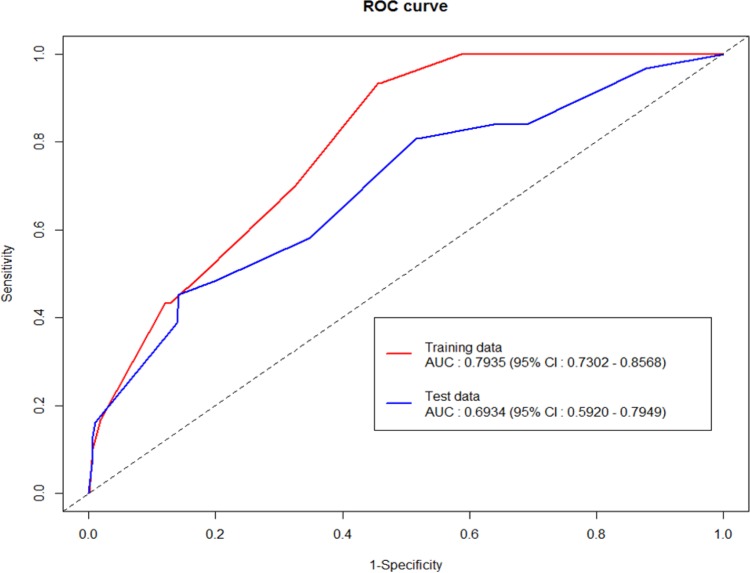
Results: Overall, LNM was observed in 5.2% (61) of 1169 patients. Four risk factors [Female sex, tumor size ≥ 3.2 cm, muscularis mucosa (M3) invasion, and lymphatic-vascular involvement] were significantly associated with LNM, which were incorporated into the RSS. The area under the receiver operating characteristic curve for predicting LNM after internal validation was 0.69 [95% confidence interval (CI), 0.59-0.79]. A total score of 2 points corresponded to the optimal RSS threshold with a discrimination of 0.75 (95% CI 0.69-0.81). The LNM rates were 1.6% for low risk (<2 points) and 8.9% for high-risk (≥2 points) patients, with a negative predictive value of 98.6% (95% CI 0.98-1.00).
Conclusions: A RSS could be useful in clinical practice to determine which patients with intramucosal PDC have low risk of LNM.
Conflict of interest statement
Figures
Similar articles
-
A Risk-prediction Model Based on Lymph-node Metastasis for Incorporation Into a Treatment Algorithm for Signet Ring Cell-type Intramucosal Gastric Cancer.Ann Surg. 2016 Dec;264(6):1038-1043. doi: 10.1097/SLA.0000000000001602. Ann Surg. 2016. PMID: 27828821
-
Indication for endoscopic treatment based on the risk of lymph node metastasis in patients with undifferentiated early gastric cancer.Asian J Surg. 2020 Oct;43(10):973-977. doi: 10.1016/j.asjsur.2019.12.002. Epub 2020 Jan 18. Asian J Surg. 2020. PMID: 31964584
-
Intramucosal gastric cancer: the rate of lymph node metastasis in signet ring cell carcinoma is as low as that in well-differentiated adenocarcinoma.Eur J Gastroenterol Hepatol. 2015 Feb;27(2):170-4. doi: 10.1097/MEG.0000000000000258. Eur J Gastroenterol Hepatol. 2015. PMID: 25503738
-
The incidence of lymph node metastasis in early gastric cancer according to the expanded criteria in comparison with the absolute criteria of the Japanese Gastric Cancer Association: a systematic review of the literature and meta-analysis.Gastrointest Endosc. 2018 Feb;87(2):338-347. doi: 10.1016/j.gie.2017.09.025. Epub 2017 Sep 28. Gastrointest Endosc. 2018. PMID: 28966062 Review.
-
Predictive factors of lymph node metastasis in undifferentiated early gastric cancers and application of endoscopic mucosal resection.Surg Oncol. 2010 Dec;19(4):221-6. doi: 10.1016/j.suronc.2009.05.006. Epub 2010 May 14. Surg Oncol. 2010. PMID: 20471826 Review.
Cited by
-
Predictive Factors for Lymph Node Metastasis in Undifferentiated Early Gastric Cancer: a Systematic Review and Meta-analysis.J Gastrointest Surg. 2017 Apr;21(4):700-711. doi: 10.1007/s11605-017-3364-7. Epub 2017 Jan 24. J Gastrointest Surg. 2017. PMID: 28120275 Review.
-
Machine learning predicts lymph node metastasis of poorly differentiated-type intramucosal gastric cancer.Sci Rep. 2021 Jan 14;11(1):1300. doi: 10.1038/s41598-020-80582-w. Sci Rep. 2021. PMID: 33446730 Free PMC article.
-
Inverse correlation between Interleukin-34 and gastric cancer, a potential biomarker for prognosis.Cell Biosci. 2020 Aug 4;10:94. doi: 10.1186/s13578-020-00454-8. eCollection 2020. Cell Biosci. 2020. PMID: 32765828 Free PMC article.
-
Clinical implications of interleukins-31, 32, and 33 in gastric cancer.World J Gastrointest Oncol. 2022 Sep 15;14(9):1808-1822. doi: 10.4251/wjgo.v14.i9.1808. World J Gastrointest Oncol. 2022. PMID: 36187404 Free PMC article.
-
Outcomes of Endoscopic Submucosal Dissection for Early Gastric Cancer with Undifferentiated-Type Histology: A Clinical Simulation Using a Non-Selected Surgical Cohort.Gut Liver. 2018 May 15;12(3):263-270. doi: 10.5009/gnl17247. Gut Liver. 2018. PMID: 29271182 Free PMC article.
References
-
- Gotoda T, Yanagisawa A, Sasako M, Ono H, Nakanishi Y, Shimoda T, et al. Incidence of lymph node metastasis from early gastric cancer: estimation with a large number of cases at two large centers. Gastric Cancer. 2000;3: 219–225. - PubMed
-
- Ishikawa S, Togashi A, Inoue M, Honda S, Nozawa F, Toyama E, et al. Indications for EMR/ESD in cases of early gastric cancer: relationship between histological type, depth of wall invasion, and lymph node metastasis. Gastric Cancer. 2007;10: 35–38. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
