

Fibroscan improves the diagnosis sensitivity of liver fibrosis in patients with chronic hepatitis B
- PMID: 27168788
- PMCID: PMC4840545
- DOI: 10.3892/etm.2016.3135
Fibroscan improves the diagnosis sensitivity of liver fibrosis in patients with chronic hepatitis B
Abstract
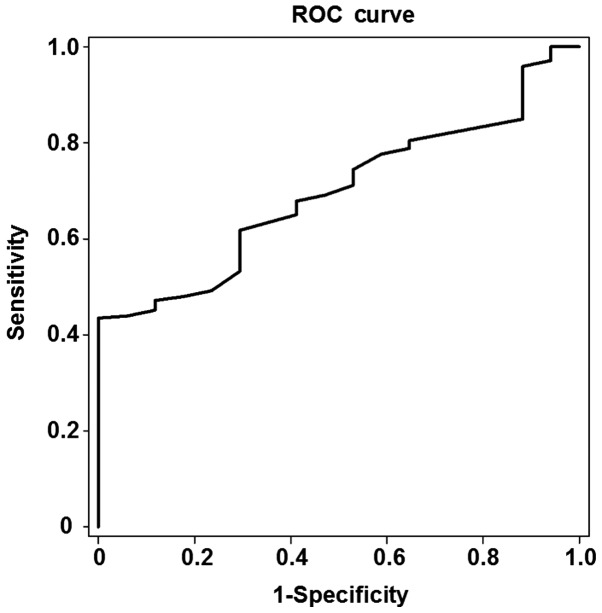
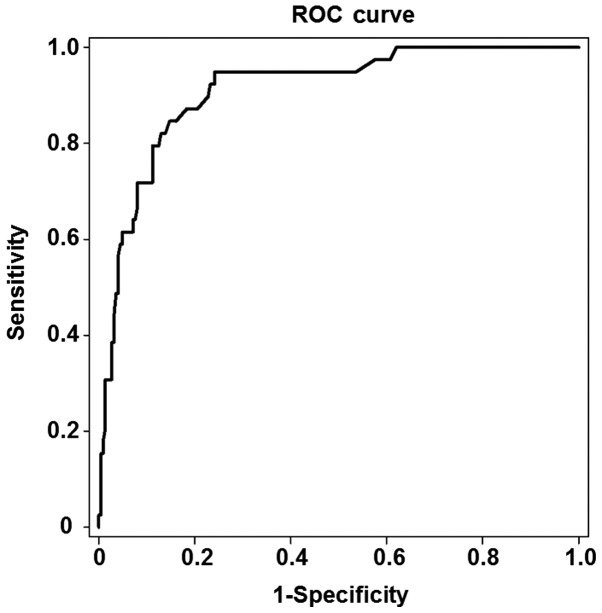
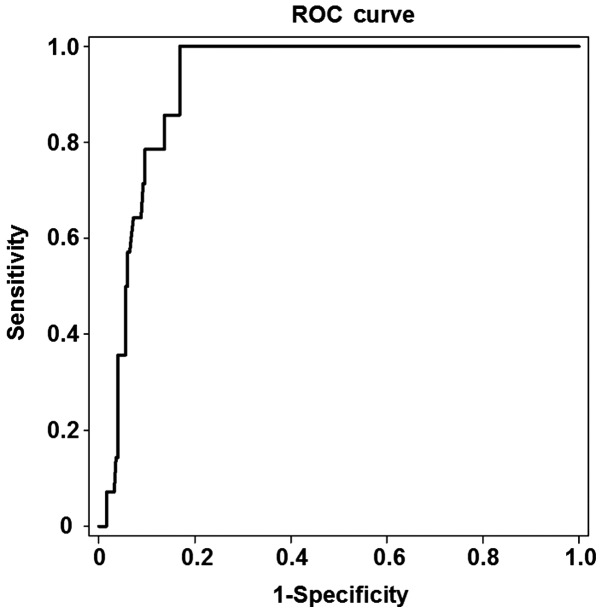
The aim of the present study was to investigate the diagnostic accuracy of Fibroscan for liver fibrosis in patients with chronic hepatitis B (CHB) with alanine aminotransferase (ALT) levels <2 times the upper normal limit. A total of 263 consecutive patients with CHB and ALT levels <2 times the upper normal limit were enrolled in the present study. Liver biopsies and liver stiffness measurements (LSM) were conducted. Receiver operating characteristic (ROC) analysis was used to determine the predictive ability of LSM for the development of liver fibrosis in patients with stage S1, S2 and S3 liver fibrosis. Bivariate Spearman rank correlation analysis was performed in order to determine the association between liver stiffness value, which was measured by Fibroscan, and liver fibrosis stage, which was measured by liver biopsy. The liver stiffness value was found to be positively correlated with the liver fibrosis stage (r=0.522, P<0.001) and necroinflammatory activity (r=0.461, P<0.001), which was measured by liver biopsy. The optimal cut-off value in the patients with stage S1, S2 and S3 liver fibrosis was 5.5, 8.0 and 10.95 kPa, respectively. The area under the ROC curve for the prediction of the development of liver fibrosis in these patients was 0.696, 0.911 and 0.923, respectively. The threshold of the optimal cut-off value exhibited a high sensitivity and specificity. The results of the present study suggested that Fibroscan may improve the sensitivity of the diagnosis of liver fibrosis in patients with CHB and ALT levels <2 times the upper normal limit, and that this sensitivity may increase with the progression of liver fibrosis.
Keywords: chronic hepatitis B; fibroscan; liver fibrosis; liver stiffness measurement.
Figures
Similar articles
-
Fibroscan can avoid liver biopsy in Indian patients with chronic hepatitis B.J Gastroenterol Hepatol. 2013 Nov;28(11):1738-45. doi: 10.1111/jgh.12318. J Gastroenterol Hepatol. 2013. PMID: 23808910
-
[Role of FibroScan in liver fibrosis evaluation in patients with chronic hepatitis B virus infection and related influencing factors].Zhonghua Gan Zang Bing Za Zhi. 2016 Sep 20;24(9):659-664. doi: 10.3760/cma.j.issn.1007-3418.2016.09.005. Zhonghua Gan Zang Bing Za Zhi. 2016. PMID: 27788721 Chinese.
-
[Correlation of FibroTouch and FibroScan with the stage of primary biliary cirrhosis].Zhonghua Gan Zang Bing Za Zhi. 2016 Dec 20;24(12):902-906. doi: 10.3760/cma.j.issn.1007-3418.2016.12.005. Zhonghua Gan Zang Bing Za Zhi. 2016. PMID: 28073410 Chinese.
-
Diagnostic efficacy of FibroScan for liver inflammation in patients with chronic hepatitis B: a single-center study with 1185 liver biopsies as controls.BMC Gastroenterol. 2022 Jan 29;22(1):37. doi: 10.1186/s12876-022-02108-0. BMC Gastroenterol. 2022. PMID: 35090390 Free PMC article.
-
[Correlation of liver stiffness measured by FibroTouch and FibroScan with Ishak fibrosis score in patients with chronic hepatitis B].Zhonghua Gan Zang Bing Za Zhi. 2017 Feb 20;25(2):145-150. doi: 10.3760/cma.j.issn.1007-3418.2017.02.013. Zhonghua Gan Zang Bing Za Zhi. 2017. PMID: 28297803 Chinese.
Cited by
-
Performance of common imaging techniques vs serum biomarkers in assessing fibrosis in patients with chronic hepatitis B: A systematic review and meta-analysis.World J Clin Cases. 2019 Aug 6;7(15):2022-2037. doi: 10.12998/wjcc.v7.i15.2022. World J Clin Cases. 2019. PMID: 31423434 Free PMC article.
-
Treatment for Viral Hepatitis as Secondary Prevention for Hepatocellular Carcinoma.Cells. 2021 Nov 9;10(11):3091. doi: 10.3390/cells10113091. Cells. 2021. PMID: 34831314 Free PMC article. Review.
-
Transient Elastography for Significant Liver Fibrosis and Cirrhosis in Chronic Hepatitis B: A Meta-Analysis.Can J Gastroenterol Hepatol. 2018 May 24;2018:3406789. doi: 10.1155/2018/3406789. eCollection 2018. Can J Gastroenterol Hepatol. 2018. PMID: 29977884 Free PMC article. Review.
-
Predictive performance of eLIFT for liver inflammation and fibrosis in chronic liver diseases.Int J Med Sci. 2021 Aug 27;18(15):3599-3608. doi: 10.7150/ijms.62386. eCollection 2021. Int J Med Sci. 2021. PMID: 34522187 Free PMC article.
-
Gamma-Glutamyl Transpeptidase-to-Platelet ratio predicts liver fibrosis in patients with concomitant chronic hepatitis B and nonalcoholic fatty liver disease.J Clin Lab Anal. 2022 Aug;36(8):e24596. doi: 10.1002/jcla.24596. Epub 2022 Jul 9. J Clin Lab Anal. 2022. PMID: 35808928 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources