

Neuropathic pain: an updated grading system for research and clinical practice
- PMID: 27115670
- PMCID: PMC4949003
- DOI: 10.1097/j.pain.0000000000000492
Neuropathic pain: an updated grading system for research and clinical practice
Abstract
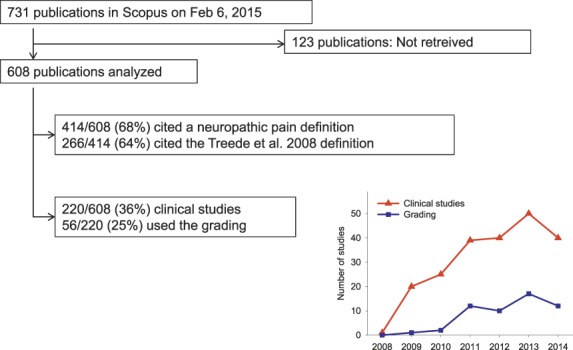
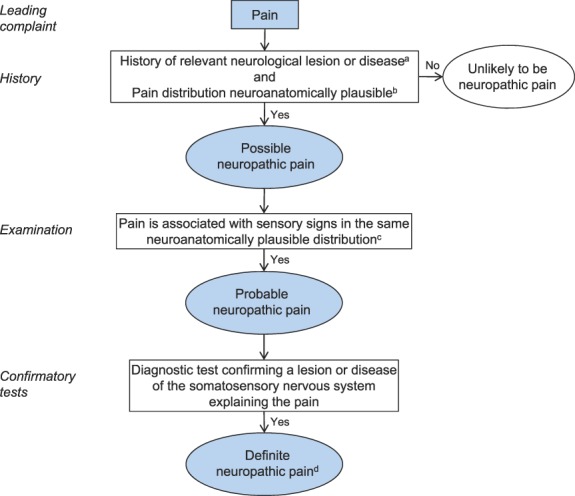
The redefinition of neuropathic pain as "pain arising as a direct consequence of a lesion or disease affecting the somatosensory system," which was suggested by the International Association for the Study of Pain (IASP) Special Interest Group on Neuropathic Pain (NeuPSIG) in 2008, has been widely accepted. In contrast, the proposed grading system of possible, probable, and definite neuropathic pain from 2008 has been used to a lesser extent. Here, we report a citation analysis of the original NeuPSIG grading paper of 2008, followed by an analysis of its use by an expert panel and recommendations for an improved grading system. As of February, 2015, 608 eligible articles in Scopus cited the paper, 414 of which cited the neuropathic pain definition. Of 220 clinical studies citing the paper, 56 had used the grading system. The percentage using the grading system increased from 5% in 2009 to 30% in 2014. Obstacles to a wider use of the grading system were identified, including (1) questions about the relative significance of confirmatory tests, (2) the role of screening tools, and (3) uncertainties about what is considered a neuroanatomically plausible pain distribution. Here, we present a revised grading system with an adjusted order, better reflecting clinical practice, improvements in the specifications, and a word of caution that even the "definite" level of neuropathic pain does not always indicate causality. In addition, we add a table illustrating the area of pain and sensory abnormalities in common neuropathic pain conditions and propose areas for further research.
Conflict of interest statement
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
Similar articles
-
Field testing of the revised neuropathic pain grading system in a cohort of patients with neck and upper limb pain.Scand J Pain. 2019 Jul 26;19(3):523-532. doi: 10.1515/sjpain-2018-0348. Scand J Pain. 2019. PMID: 30901318
-
Revised definition of neuropathic pain and its grading system: an open case series illustrating its use in clinical practice.Am J Med. 2009 Oct;122(10 Suppl):S3-12. doi: 10.1016/j.amjmed.2009.04.005. Am J Med. 2009. PMID: 19801050
-
Assessing neuropathic pain in patients with low back-related leg pain: Comparing the painDETECT Questionnaire with the 2016 NeuPSIG grading system.Eur J Pain. 2018 Jul;22(6):1160-1169. doi: 10.1002/ejp.1204. Epub 2018 Mar 2. Eur J Pain. 2018. PMID: 29436056
-
Neuropathic pain: redefinition and a grading system for clinical and research purposes.Neurology. 2008 Apr 29;70(18):1630-5. doi: 10.1212/01.wnl.0000282763.29778.59. Epub 2007 Nov 14. Neurology. 2008. PMID: 18003941
-
NeuPSIG guidelines on neuropathic pain assessment.Pain. 2011 Jan;152(1):14-27. doi: 10.1016/j.pain.2010.07.031. Epub 2010 Sep 19. Pain. 2011. PMID: 20851519 Review.
Cited by
-
ADvAnced PhysioTherapy in MuSculosKeletal Triage: Investigating prognostic factors, healthcare utilisation and clinical outcomes (ADAPT MSK) - a cohort study protocol.HRB Open Res. 2025 Jan 23;6:73. doi: 10.12688/hrbopenres.13769.1. eCollection 2023. HRB Open Res. 2025. PMID: 38384973 Free PMC article.
-
Central Sensitization in Patients with Chronic Pain Secondary to Carpal Tunnel Syndrome and Determinants.J Pain Res. 2023 Dec 19;16:4353-4366. doi: 10.2147/JPR.S441786. eCollection 2023. J Pain Res. 2023. PMID: 38145037 Free PMC article.
-
Differential effects of epidermal growth factor receptor inhibitors in a single patient with neuropathic pain.BMJ Case Rep. 2021 Mar 26;14(3):e239385. doi: 10.1136/bcr-2020-239385. BMJ Case Rep. 2021. PMID: 33771774 Free PMC article.
-
Modern Principles of Diagnosis and Treatment in Complex Regional Pain Syndrome.Dtsch Arztebl Int. 2022 Dec 27;119(51-52):879-886. doi: 10.3238/arztebl.m2022.0358. Dtsch Arztebl Int. 2022. PMID: 36482756 Free PMC article.
-
Oral herbal medicine for treatment of postherpetic neuralgia: A protocol for systematic review and meta-analysis.Medicine (Baltimore). 2022 Dec 30;101(52):e32484. doi: 10.1097/MD.0000000000032484. Medicine (Baltimore). 2022. PMID: 36595985 Free PMC article.
References
-
- Bennett DL, Woods CG. Painful and painless channelopathies. Lancet Neurol 2014;13:587–99. - PubMed
-
- Bennett M. The LANSS Pain Scale: the Leeds assessment of neuropathic symptoms and signs. PAIN 2001;92:147–57. - PubMed
-
- Bennett MI, Attal N, Backonja MM, Baron R, Bouhassira D, Freynhagen R, Scholz J, Tolle TR, Wittchen HU, Jensen TS. Using screening tools to identify neuropathic pain. PAIN 2007;127:199–203. - PubMed
-
- Bennett MI, Rayment C, Hjermstad M, Aass N, Caraceni A, Kaasa S. Prevalence and aetiology of neuropathic pain in cancer patients: a systematic review. PAIN 2012;153:359–65. - PubMed
-
- Birklein F, O'Neill D, Schlereth T. Complex regional pain syndrome: An optimistic perspective. Neurology 2015;84:89–96. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
