

Radiotherapy with concurrent temozolomide for the management of extraneural metastases in pituitary carcinoma
- PMID: 27106209
- PMCID: PMC5215904
- DOI: 10.1007/s11102-016-0721-6
Radiotherapy with concurrent temozolomide for the management of extraneural metastases in pituitary carcinoma
Abstract
Background: Pituitary carcinomas (PC) are uncommon neuroendocrine tumors, accounting for 0.1 % of all pituitary tumors. The diagnosis of PC is based on the presence of metastases from a pituitary adenoma, and not by local invasion or pathological features alone. PC is typically resistant to therapy, with a median overall survival of only 31 months. There is no standard treatment for PC, but maximal safe resection and radiation are performed when possible. Encouraging preliminary data on the use of temozolomide (TMZ)-based therapy has been previously reported.
Methods: We report the response to therapy and safety of radiation with concurrent temozolomide (RT/TMZ) in 2 adult patients with heavily pretreated PC and extraneural metastases.
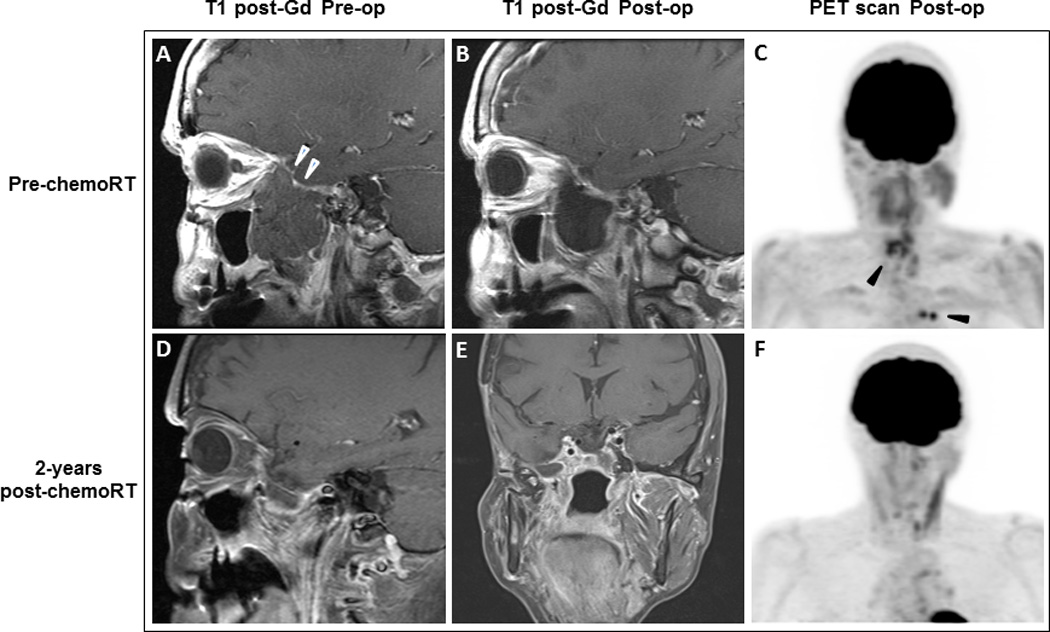
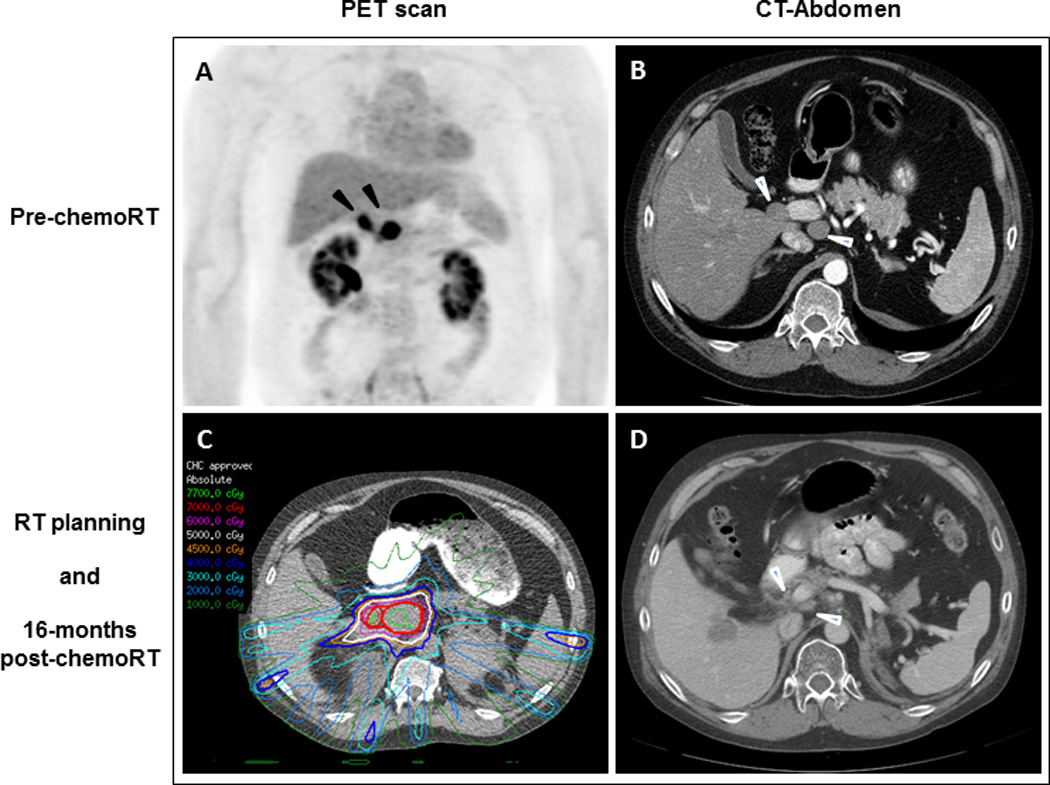
Results: Both patients had prior history of pituitary macroadenoma. At the time of diagnosis of PC, Ki-67 % was 24.2 and 10 %, with positive p53 staining in one case. Metastatic sites included lymph nodes, liver and bone. Case-1 received RT/TMZ to the tumor bed in the skull base and to the metastases in the cervical lymph nodes. Case-2 received RT/TMZ to recurrent tumor involving portacaval lymph nodes. Both patients achieved excellent long-term control of the sites of treated extraneural metastases, with no significant acute or delayed toxicity.
Conclusions: RT/TMZ was safely delivered and might provide sustained control of extraneural metastases in PC. Although this retrospective report has limitations, RT/TMZ can be considered as a therapeutic option for the management of extraneural metastases in PC.
Keywords: Capecitabine; Chemoradiation; Pituitary carcinoma; Pituitary macroadenoma; Temozolomide.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Similar articles
-
Successful treatment of pituitary carcinoma with concurrent radiation, temozolomide, and bevacizumab after resection.J Clin Neurosci. 2017 Jul;41:75-77. doi: 10.1016/j.jocn.2017.02.052. Epub 2017 Mar 11. J Clin Neurosci. 2017. PMID: 28291643
-
Treatment of aggressive pituitary tumours and carcinomas: results of a European Society of Endocrinology (ESE) survey 2016.Eur J Endocrinol. 2018 Mar;178(3):265-276. doi: 10.1530/EJE-17-0933. Epub 2018 Jan 12. Eur J Endocrinol. 2018. PMID: 29330228
-
Treatment of pituitary carcinomas and atypical pituitary adenomas: a review.Neurol Med Chir (Tokyo). 2014;54(12):966-73. doi: 10.2176/nmc.ra.2014-0178. Epub 2014 Nov 29. Neurol Med Chir (Tokyo). 2014. PMID: 25446382 Free PMC article. Review.
-
DNA mismatch repair protein (MSH6) correlated with the responses of atypical pituitary adenomas and pituitary carcinomas to temozolomide: the national cooperative study by the Japan Society for Hypothalamic and Pituitary Tumors.J Clin Endocrinol Metab. 2013 Mar;98(3):1130-6. doi: 10.1210/jc.2012-2924. Epub 2013 Jan 30. J Clin Endocrinol Metab. 2013. PMID: 23365123
-
Temozolomide responsiveness in aggressive corticotroph tumours: a case report and review of the literature.Pituitary. 2012 Sep;15(3):276-87. doi: 10.1007/s11102-011-0363-7. Pituitary. 2012. PMID: 22076588 Review.
Cited by
-
Delayed Craniospinal Metastasis of Aggressive Nonfunctioning Pituitary Adenomas as Pituitary Carcinomas.J Neurol Surg B Skull Base. 2021 Mar 1;83(Suppl 2):e253-e259. doi: 10.1055/s-0041-1725024. eCollection 2022 Jun. J Neurol Surg B Skull Base. 2021. PMID: 35832993 Free PMC article.
-
Case Report: Progression of a Silent Corticotroph Tumor to an Aggressive Secreting Corticotroph Tumor, Treated by Temozolomide. Changes in the Clinic, the Pathology, and the β-Catenin and α-SMA Expression.Front Endocrinol (Lausanne). 2022 Jul 19;13:870172. doi: 10.3389/fendo.2022.870172. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35928898 Free PMC article.
-
Malignant transformation in non-functioning pituitary adenomas (pituitary carcinoma).Pituitary. 2018 Apr;21(2):217-229. doi: 10.1007/s11102-017-0857-z. Pituitary. 2018. PMID: 29299820 Review.
-
Detection of circulating tumor cells in patients with pituitary tumors.BMC Cancer. 2018 Mar 27;18(1):336. doi: 10.1186/s12885-018-4162-7. BMC Cancer. 2018. PMID: 29587659 Free PMC article.
-
Incidence, demographics, and survival of patients with primary pituitary tumors: a SEER database study in 2004-2016.Sci Rep. 2021 Jul 26;11(1):15155. doi: 10.1038/s41598-021-94658-8. Sci Rep. 2021. PMID: 34312470 Free PMC article.
References
-
- Scheithauer BW, Kovacs KT, Laws ER, Jr, Randall RV. Pathology of invasive pituitary tumors with special reference to functional classification. J Neurosurg. 1986;65(6):733–744. - PubMed
-
- Thapar K, Scheithauer BW, Kovacs K, Pernicone PJ, Laws ER., Jr p53 expression in pituitary adenomas and carcinomas: correlation with invasiveness and tumor growth fractions. Neurosurgery. 1996;38(4):765–770. discussion 770-771. - PubMed
-
- Kaltsas GA, Nomikos P, Kontogeorgos G, Buchfelder M, Grossman AB. Clinical review: Diagnosis and management of pituitary carcinomas. J Clin Endocrinol Metab. 2005;90(5):3089–3099. - PubMed
-
- McCutcheon IE, Pieper DR, Fuller GN, Benjamin RS, Friend KE, Gagel RF. Pituitary carcinoma containing gonadotropins: treatment by radical excision and cytotoxic chemotherapy: case report. Neurosurgery. 2000;46(5):1233–1239. discussion 1239-1240. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
