

Characteristics and outcomes of anti-infective de-escalation during health care-associated intra-abdominal infections
- PMID: 27052675
- PMCID: PMC4823898
- DOI: 10.1186/s13054-016-1267-8
Characteristics and outcomes of anti-infective de-escalation during health care-associated intra-abdominal infections
Abstract
Background: De-escalation is strongly recommended for antibiotic stewardship. No studies have addressed this issue in the context of health care-associated intra-abdominal infections (HCIAI). We analyzed the factors that could interfere with this process and their clinical consequences in intensive care unit (ICU) patients with HCIAI.
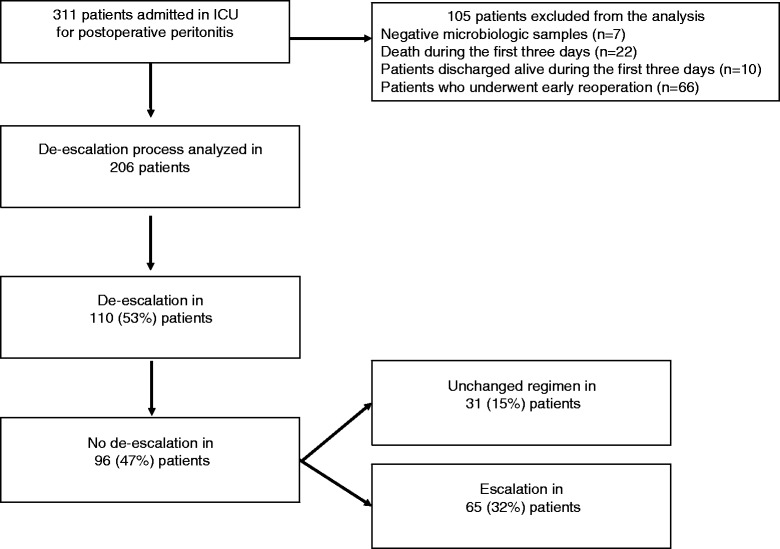
Methods: All consecutive patients admitted for the management of HCIAI who survived more than 3 days following their diagnosis, who remained in the ICU for more than 3 days, and who did not undergo early reoperation during the first 3 days were analyzed prospectively in an observational, single-center study in a tertiary care university hospital.
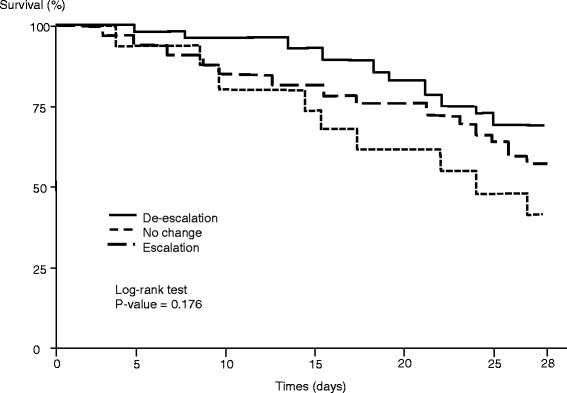
Results: Overall, 311 patients with HCIAI were admitted to the ICU. De-escalation was applied in 110 patients (53%), and no de-escalation was reported in 96 patients (47%) (escalation in 65 [32%] and unchanged regimen in 31 [15%]). Lower proportions of Enterococcus faecium, nonfermenting Gram-negative bacilli (NFGNB), and multidrug-resistant (MDR) strains were cultured in the de-escalation group. No clinical difference was observed at day 7 between patients who were de-escalated and those who were not. Determinants of de-escalation in multivariate analysis were adequate empiric therapy (OR 9.60, 95% CI 4.02-22.97) and empiric use of vancomycin (OR 3.39, 95% CI 1.46-7.87), carbapenems (OR 2.64, 95% CI 1.01-6.91), and aminoglycosides (OR 2.31 95% CI 1.08-4.94). The presence of NFGNB (OR 0.28, 95% CI 0.09-0.89) and the presence of MDR bacteria (OR 0.21, 95% CI 0.09-0.52) were risk factors for non-de-escalation. De-escalation did not change the overall duration of therapy. The risk factors for death at day 28 were presence of fungi (HR 2.64, 95% CI 1.34-5.17), Sequential Organ Failure Assessment score on admission (HR 1.29, 95% CI 1.16-1.42), and age (HR 1.03, 95% CI 1.01-1.05). The survival rate expressed by a Kaplan-Meier curve was similar between groups (log-rank test p value 0.176).
Conclusions: De-escalation is a feasible option in patients with polymicrobial infections such as HCIAI, but MDR organisms and NFGNB limit its implementation.
Keywords: Antibiotic therapy; De-escalation; Health care-associated intra-abdominal infections; Multidrug-resistant bacteria; Peritonitis.
Figures
Similar articles
-
Clinical characteristics and prognosis of bacteraemia during postoperative intra-abdominal infections.Crit Care. 2018 Jul 7;22(1):175. doi: 10.1186/s13054-018-2099-5. Crit Care. 2018. PMID: 29980218 Free PMC article.
-
Antimicrobial de-escalation strategies in hospitalized patients with pneumonia, intra-abdominal infections, and bacteremia.J Hosp Med. 2012;7 Suppl 1:S13-21. doi: 10.1002/jhm.983. J Hosp Med. 2012. PMID: 23737333 Review.
-
Antimicrobial de-escalation strategies in hospitalized patients with pneumonia, intra-abdominal infections, and bacteremia.J Hosp Med. 2012;7 Suppl 1:S13-21. doi: 10.1002/jhm.983. J Hosp Med. 2012. PMID: 23677630 Review.
-
Inclusion of Vancomycin as Part of Broad-Spectrum Coverage Does Not Improve Outcomes in Patients with Intra-Abdominal Infections: A Post Hoc Analysis.Surg Infect (Larchmt). 2016 Dec;17(6):694-699. doi: 10.1089/sur.2016.095. Epub 2016 Aug 2. Surg Infect (Larchmt). 2016. PMID: 27483362
-
Strategies of initiation and streamlining of antibiotic therapy in 41 French intensive care units.Crit Care. 2011;15(1):R17. doi: 10.1186/cc9961. Epub 2011 Jan 13. Crit Care. 2011. PMID: 21232098 Free PMC article.
Cited by
-
Feasibility of Antimicrobial Stewardship (AMS) in Critical Care Settings: A Multidisciplinary Approach Strategy.Med Sci (Basel). 2018 May 25;6(2):40. doi: 10.3390/medsci6020040. Med Sci (Basel). 2018. PMID: 29799500 Free PMC article.
-
Short-course antibiotic therapy for critically ill patients treated for postoperative intra-abdominal infection: the DURAPOP randomised clinical trial.Intensive Care Med. 2018 Mar;44(3):300-310. doi: 10.1007/s00134-018-5088-x. Epub 2018 Feb 26. Intensive Care Med. 2018. PMID: 29484469 Clinical Trial.
-
Optimized Treatment of Nosocomial Peritonitis.Antibiotics (Basel). 2023 Dec 8;12(12):1711. doi: 10.3390/antibiotics12121711. Antibiotics (Basel). 2023. PMID: 38136745 Free PMC article. Review.
-
What's new in multidrug-resistant pathogens in the ICU?Ann Intensive Care. 2016 Dec;6(1):96. doi: 10.1186/s13613-016-0199-4. Epub 2016 Oct 6. Ann Intensive Care. 2016. PMID: 27714706 Free PMC article. Review.
-
Confounding by indication of the safety of de-escalation in community-acquired pneumonia: A simulation study embedded in a prospective cohort.PLoS One. 2019 Sep 27;14(9):e0218062. doi: 10.1371/journal.pone.0218062. eCollection 2019. PLoS One. 2019. PMID: 31560686 Free PMC article.
References
-
- Weiss E, Zahar JR, Lesprit P, Ruppe E, Leone M, Chastre J, et al. Elaboration of a consensual definition of de-escalation allowing a ranking of β-lactams. Clin Microbiol Infect. 2015;21:649.e1–10. - PubMed
-
- Dellit TH, Owens RC, McGowan JE, Jr, Gerding DN, Weinstein RA, Burke JP, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis. 2007;44:159–77. doi: 10.1086/510393. - DOI - PubMed
-
- Garnacho-Montero J, Gutiérrez-Pizarraya A, Escoresca-Ortega A, Corcia-Palomo Y, Fernández-Delgado E, Herrera-Melero I, et al. De-escalation of empirical therapy is associated with lower mortality in patients with severe sepsis and septic shock. Intensive Care Med. 2014;40:32–40. doi: 10.1007/s00134-013-3077-7. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
