

Niclosamide enhances abiraterone treatment via inhibition of androgen receptor variants in castration resistant prostate cancer
- PMID: 27049719
- PMCID: PMC5078008
- DOI: 10.18632/oncotarget.8493
Niclosamide enhances abiraterone treatment via inhibition of androgen receptor variants in castration resistant prostate cancer
Erratum in
-
Correction: Niclosamide enhances abiraterone treatment via inhibition of androgen receptor variants in castration resistant prostate cancer.Oncotarget. 2024 Oct 1;15:677-678. doi: 10.18632/oncotarget.28656. Oncotarget. 2024. PMID: 39352799 Free PMC article. No abstract available.
Abstract
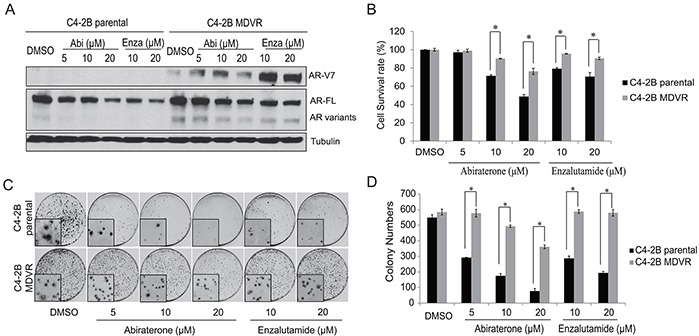
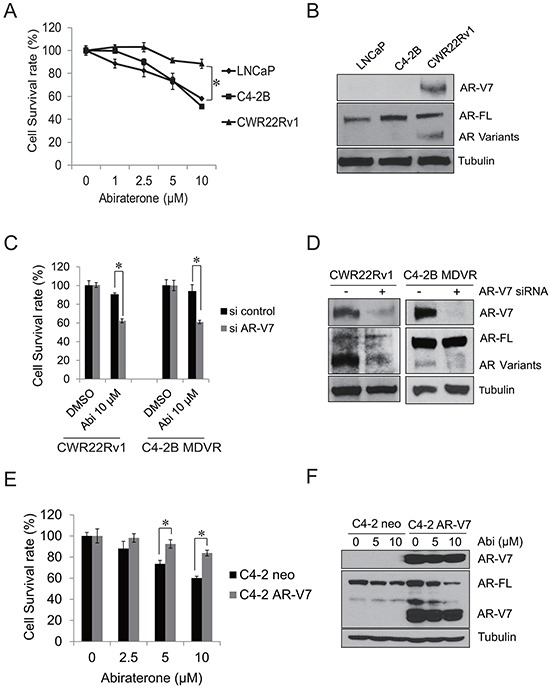
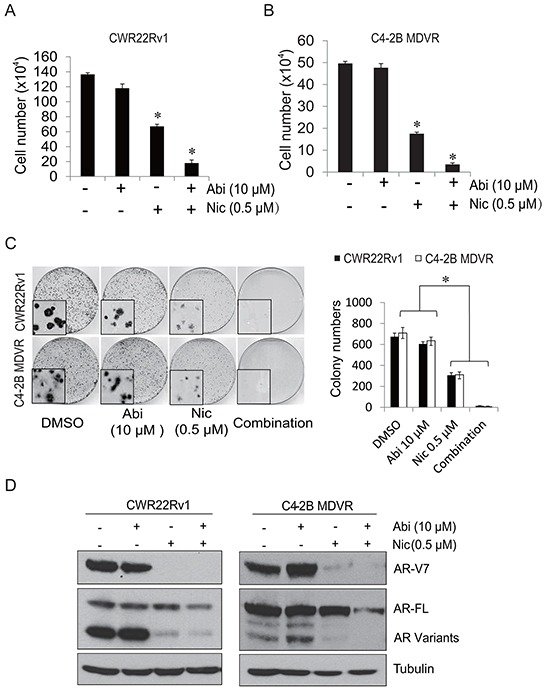
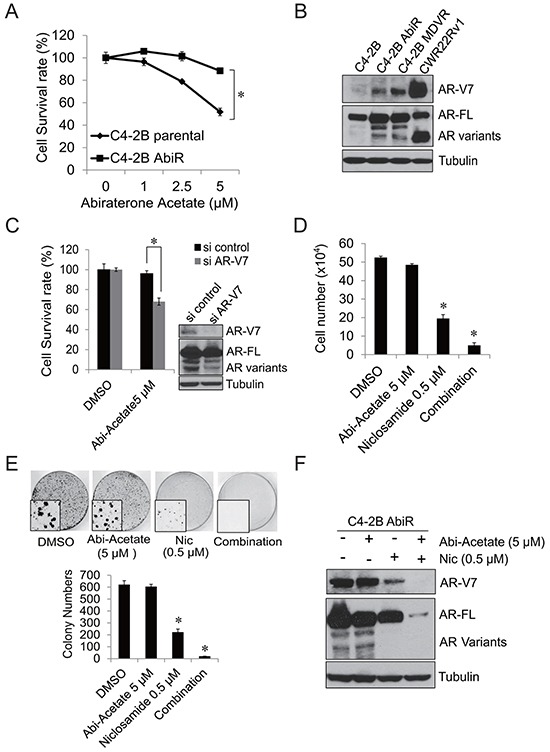
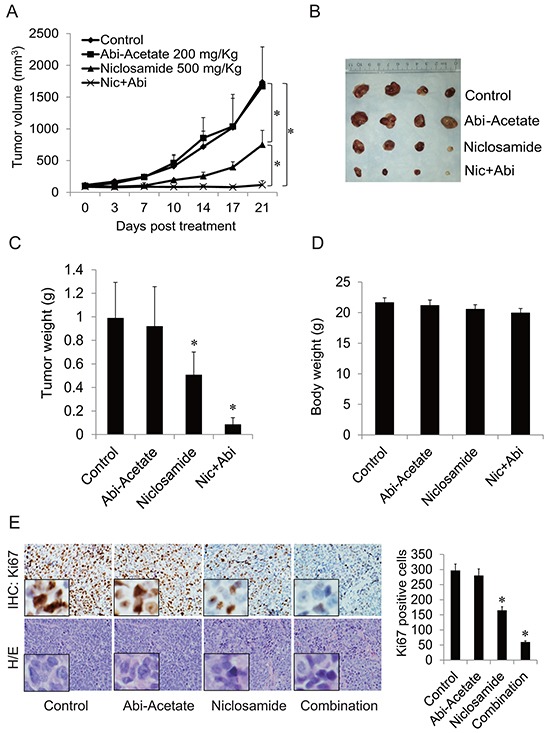
Considerable evidence from both clinical and experimental studies suggests that androgen receptor variants, particularly androgen receptor variant 7 (AR-V7), are critical in the induction of resistance to enzalutamide and abiraterone. In this study, we investigated the role of AR-V7 in the cross-resistance of enzalutamide and abiraterone and examined if inhibition of AR-V7 can improve abiraterone treatment response. We found that enzalutamide-resistant cells are cross-resistant to abiraterone, and that AR-V7 confers resistance to abiraterone. Knock down of AR-V7 by siRNA in abiraterone resistant CWR22Rv1 and C4-2B MDVR cells restored their sensitivity to abiraterone, indicating that AR-V7 is involved in abiraterone resistance. Abiraterone resistant prostate cancer cells generated by chronic treatment with abiraterone showed enhanced AR-V7 protein expression. Niclosamide, an FDA-approved antihelminthic drug that has been previously identified as a potent inhibitor of AR-V7, re-sensitizes resistant cells to abiraterone treatment in vitro and in vivo. In summary, this preclinical study suggests that overexpression of AR-V7 contributes to resistance to abiraterone, and supports the development of combination of abiraterone with niclosamide as a potential treatment for advanced castration resistant prostate cancer.
Keywords: abiraterone; androgen receptor variant; niclosamide; prostate cancer; resistance.
Conflict of interest statement
Patent application: C. Liu, W. Lou, and A.C. Gao are co-inventors on a patent application covering the use of niclosamide.
Figures
Similar articles
-
Niclosamide inhibits androgen receptor variants expression and overcomes enzalutamide resistance in castration-resistant prostate cancer.Clin Cancer Res. 2014 Jun 15;20(12):3198-3210. doi: 10.1158/1078-0432.CCR-13-3296. Epub 2014 Apr 16. Clin Cancer Res. 2014. PMID: 24740322 Free PMC article.
-
Niclosamide and Bicalutamide Combination Treatment Overcomes Enzalutamide- and Bicalutamide-Resistant Prostate Cancer.Mol Cancer Ther. 2017 Aug;16(8):1521-1530. doi: 10.1158/1535-7163.MCT-16-0912. Epub 2017 May 12. Mol Cancer Ther. 2017. PMID: 28500234 Free PMC article.
-
Preclinical Study using Malat1 Small Interfering RNA or Androgen Receptor Splicing Variant 7 Degradation Enhancer ASC-J9® to Suppress Enzalutamide-resistant Prostate Cancer Progression.Eur Urol. 2017 Nov;72(5):835-844. doi: 10.1016/j.eururo.2017.04.005. Epub 2017 May 18. Eur Urol. 2017. PMID: 28528814 Free PMC article.
-
Androgen receptor splice variants in the era of enzalutamide and abiraterone.Horm Cancer. 2014 Oct;5(5):265-73. doi: 10.1007/s12672-014-0190-1. Epub 2014 Jul 22. Horm Cancer. 2014. PMID: 25048254 Free PMC article. Review.
-
Targeting persistent androgen receptor signaling in castration-resistant prostate cancer.Med Oncol. 2016 May;33(5):44. doi: 10.1007/s12032-016-0759-3. Epub 2016 Apr 4. Med Oncol. 2016. PMID: 27042852 Review.
Cited by
-
High Mobility Group AT-hook 2: A Biomarker Associated with Resistance to Enzalutamide in Prostate Cancer Cells.Cancers (Basel). 2024 Jul 24;16(15):2631. doi: 10.3390/cancers16152631. Cancers (Basel). 2024. PMID: 39123360 Free PMC article.
-
Wntless promotes cellular viability and resistance to enzalutamide in castration-resistant prostate cancer cells.Am J Clin Exp Urol. 2019 Aug 15;7(4):203-214. eCollection 2019. Am J Clin Exp Urol. 2019. PMID: 31511827 Free PMC article.
-
WNT signalling in prostate cancer.Nat Rev Urol. 2017 Nov;14(11):683-696. doi: 10.1038/nrurol.2017.144. Epub 2017 Sep 12. Nat Rev Urol. 2017. PMID: 28895566 Review.
-
Protein Arginine Methyltransferase 5 Promotes pICln-Dependent Androgen Receptor Transcription in Castration-Resistant Prostate Cancer.Cancer Res. 2020 Nov 15;80(22):4904-4917. doi: 10.1158/0008-5472.CAN-20-1228. Epub 2020 Sep 30. Cancer Res. 2020. PMID: 32999000 Free PMC article.
-
Selectively Targeting Breast Cancer Stem Cells by 8-Quinolinol and Niclosamide.Int J Mol Sci. 2022 Oct 4;23(19):11760. doi: 10.3390/ijms231911760. Int J Mol Sci. 2022. PMID: 36233074 Free PMC article.
References
-
- Attard G, Reid AH, Olmos D, de Bono JS. Antitumor activity with CYP17 blockade indicates that castration-resistant prostate cancer frequently remains hormone driven. Cancer research. 2009;69:4937–4940. - PubMed
-
- Attard G, Reid AH, A'Hern R, Parker C, Oommen NB, Folkerd E, Messiou C, Molife LR, Maier G, Thompson E, Olmos D, Sinha R, Lee G, et al. Selective inhibition of CYP17 with abiraterone acetate is highly active in the treatment of castration-resistant prostate cancer. Journal of clinical oncology. 2009;27:3742–3748. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
