

Copa Syndrome: a Novel Autosomal Dominant Immune Dysregulatory Disease
- PMID: 27048656
- PMCID: PMC4842120
- DOI: 10.1007/s10875-016-0271-8
Copa Syndrome: a Novel Autosomal Dominant Immune Dysregulatory Disease
Abstract
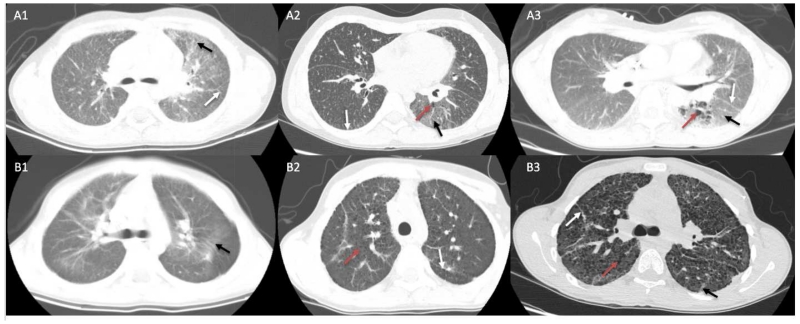
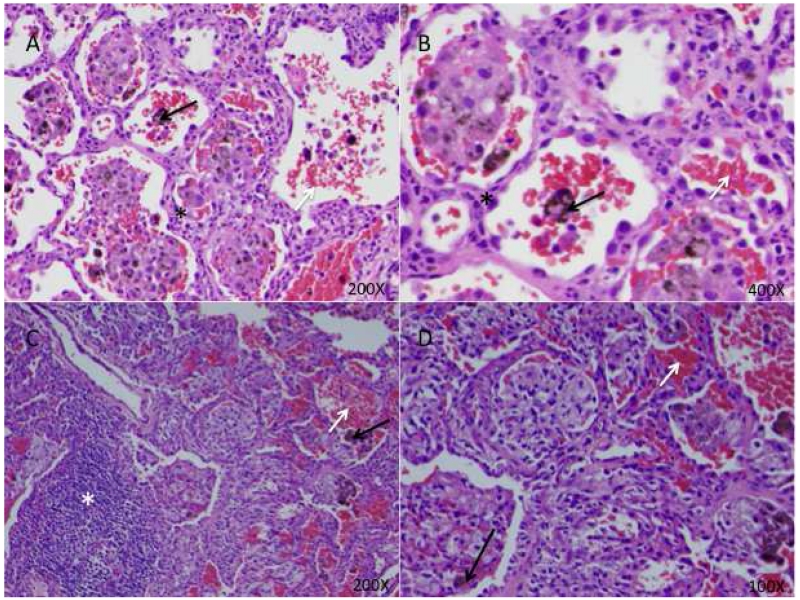
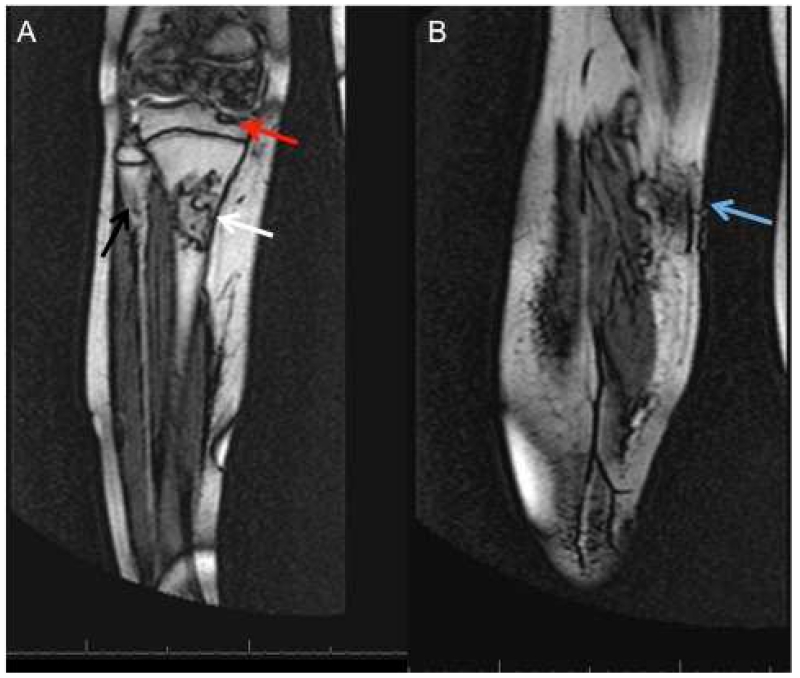
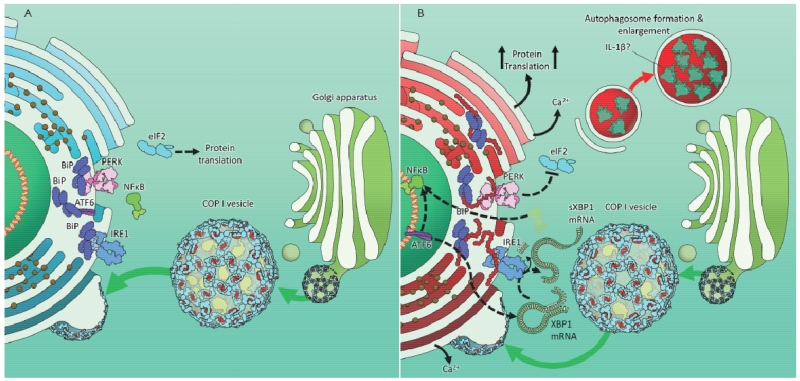
Inherently defective immunity typically results in either ineffective host defense, immune regulation, or both. As a category of primary immunodeficiency diseases, those that impair immune regulation can lead to autoimmunity and/or autoinflammation. In this review we focus on one of the most recently discovered primary immunodeficiencies that leads to immune dysregulation: "Copa syndrome". Copa syndrome is named for the gene mutated in the disease, which encodes the alpha subunit of the coatomer complex-I that, in aggregate, is devoted to transiting molecular cargo from the Golgi complex to the endoplasmic reticulum (ER). Copa syndrome is autosomal dominant with variable expressivity and results from mutations affecting a narrow amino acid stretch in the COPA gene-encoding COPα protein. Patients with these mutations typically develop arthritis and interstitial lung disease with pulmonary hemorrhage representing a striking feature. Immunologically Copa syndrome is associated with autoantibody development, increased Th17 cells and pro-inflammatory cytokine expression including IL-1β and IL-6. Insights have also been gained into the underlying mechanism of Copa syndrome, which include excessive ER stress owing to the impaired return of proteins from the Golgi, and presumably resulting aberrant cellular autophagy. As such it represents a novel cellular disorder of intracellular trafficking associated with a specific clinical presentation and phenotype.
Keywords: Autoimmunity; arthritis; autosomal dominant; interstitial lung disease; primary immunodeficiency.
Figures
Similar articles
-
Genetics of COPA syndrome.Appl Clin Genet. 2019 Feb 8;12:11-18. doi: 10.2147/TACG.S153600. eCollection 2019. Appl Clin Genet. 2019. PMID: 30804679 Free PMC article. Review.
-
COPA mutations impair ER-Golgi transport and cause hereditary autoimmune-mediated lung disease and arthritis.Nat Genet. 2015 Jun;47(6):654-60. doi: 10.1038/ng.3279. Epub 2015 Apr 20. Nat Genet. 2015. PMID: 25894502 Free PMC article.
-
An unprecedented COPA gene mutation in two patients in the same family: comparative clinical analysis of newly reported patients with other known COPA gene mutations.Pediatr Rheumatol Online J. 2019 Aug 27;17(1):59. doi: 10.1186/s12969-019-0359-9. Pediatr Rheumatol Online J. 2019. PMID: 31455335 Free PMC article. Review.
-
COPA syndrome in an Icelandic family caused by a recurrent missense mutation in COPA.BMC Med Genet. 2017 Nov 14;18(1):129. doi: 10.1186/s12881-017-0490-8. BMC Med Genet. 2017. PMID: 29137621 Free PMC article.
-
Imaging findings of COPA Syndrome.Pediatr Radiol. 2023 May;53(5):844-853. doi: 10.1007/s00247-023-05600-1. Epub 2023 Feb 7. Pediatr Radiol. 2023. PMID: 36746811
Cited by
-
Recent advances in the understanding of bronchiolitis in adults.F1000Res. 2020 Jun 8;9:F1000 Faculty Rev-568. doi: 10.12688/f1000research.21778.1. eCollection 2020. F1000Res. 2020. PMID: 32551095 Free PMC article. Review.
-
Type I Interferonopathies in Children: An Overview.Front Pediatr. 2021 Mar 31;9:631329. doi: 10.3389/fped.2021.631329. eCollection 2021. Front Pediatr. 2021. PMID: 33869112 Free PMC article. Review.
-
Etiologic spectrum of interstitial lung diseases in Chinese children older than 2 years of age.Orphanet J Rare Dis. 2020 Jan 22;15(1):25. doi: 10.1186/s13023-019-1270-7. Orphanet J Rare Dis. 2020. PMID: 31969166 Free PMC article.
-
Lung Involvement in Children with Hereditary Autoinflammatory Disorders.Int J Mol Sci. 2016 Dec 15;17(12):2111. doi: 10.3390/ijms17122111. Int J Mol Sci. 2016. PMID: 27983684 Free PMC article. Review.
-
Exome Sequencing Identifies a Novel MAP3K14 Mutation in Recessive Atypical Combined Immunodeficiency.Front Immunol. 2017 Nov 27;8:1624. doi: 10.3389/fimmu.2017.01624. eCollection 2017. Front Immunol. 2017. PMID: 29230214 Free PMC article.
References
-
- Picard C, Al-Herz W, Bousfiha A, Casanova J-L, Chatila T, Conley ME, et al. J Clin Immunol. Springer; US: 2015. Primary Immunodeficiency Diseases: an Update on the Classification from the International Union of Immunological Societies Expert Committee for Primary Immunodeficiency 2015; pp. 1–31. - PMC - PubMed
-
- Melki I, Crow YJ. Novel monogenic diseases causing human autoimmunity. Current Opinion in Immunology. 2015;37:1–5. - PubMed
-
- Sacri A-S, Chambaraud T, Ranchin B, Florkin B, Sée H, Decramer S, et al. Clinical characteristics and outcomes of childhood-onset ANCA-associated vasculitis: a French nationwide study. Nephrol. Dial. Transplant. 2015;30(Suppl 1):i104–12. - PubMed
-
- Siomou E, Tramma D, Bowen C, Milford DV. Pediatr. Nephrol. Vol. 27. Springer-Verlag; 2012. ANCA-associated glomerulonephritis/systemic vasculitis in childhood: clinical features-outcome; pp. 1911–20. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
