

An Immunohistochemical Algorithm for Ovarian Carcinoma Typing
- PMID: 26974996
- PMCID: PMC4978603
- DOI: 10.1097/PGP.0000000000000274
An Immunohistochemical Algorithm for Ovarian Carcinoma Typing
Abstract
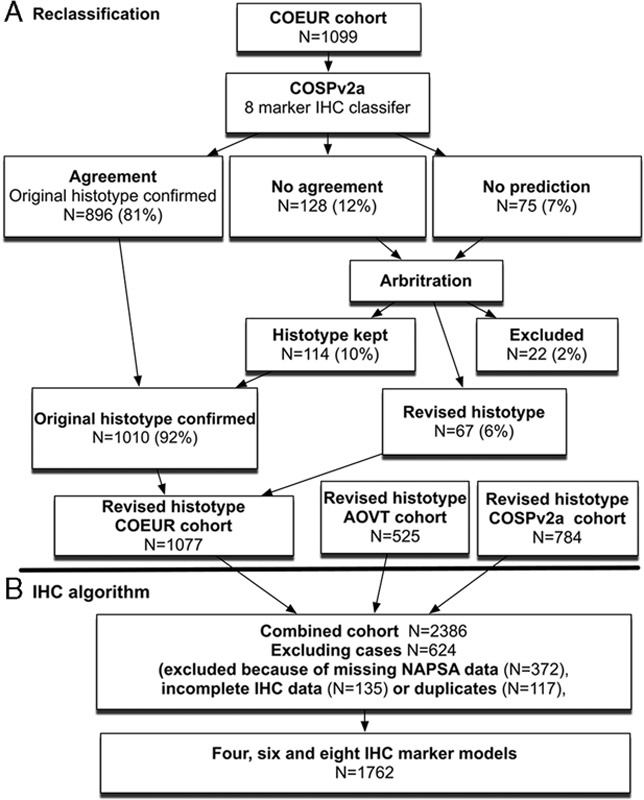
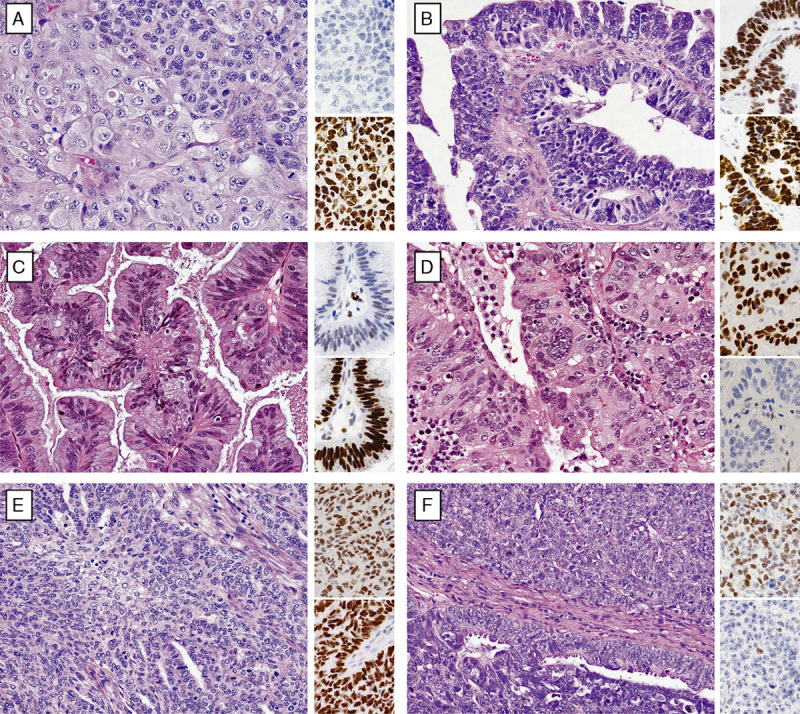
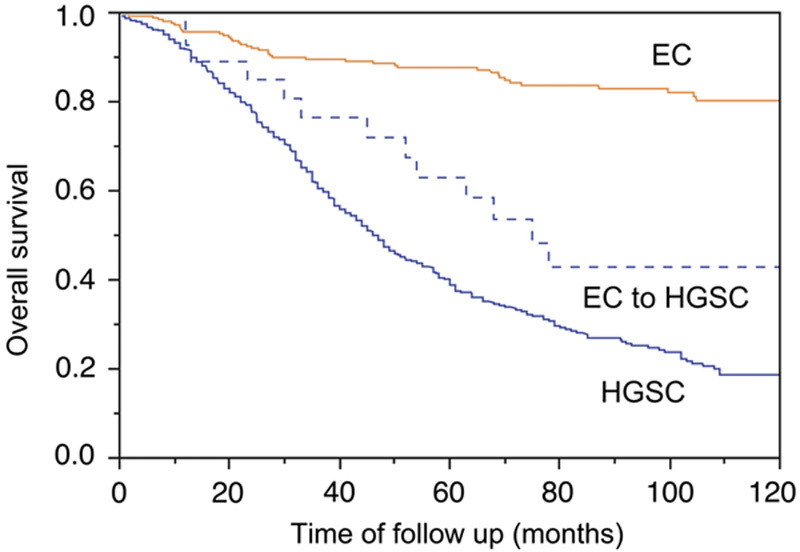
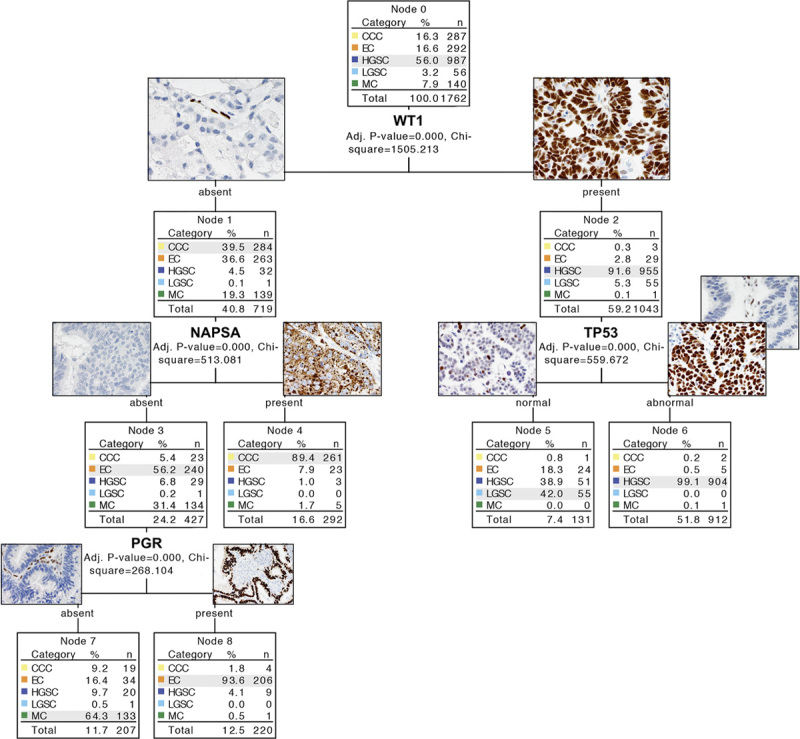
There are 5 major histotypes of ovarian carcinomas. Diagnostic typing criteria have evolved over time, and past cohorts may be misclassified by current standards. Our objective was to reclassify the recently assembled Canadian Ovarian Experimental Unified Resource and the Alberta Ovarian Tumor Type cohorts using immunohistochemical (IHC) biomarkers and to develop an IHC algorithm for ovarian carcinoma histotyping. A total of 1626 ovarian carcinoma samples from the Canadian Ovarian Experimental Unified Resource and the Alberta Ovarian Tumor Type were subjected to a reclassification by comparing the original with the predicted histotype. Histotype prediction was derived from a nominal logistic regression modeling using a previously reclassified cohort (N=784) with the binary input of 8 IHC markers. Cases with discordant original or predicted histotypes were subjected to arbitration. After reclassification, 1762 cases from all cohorts were subjected to prediction models (χ Automatic Interaction Detection, recursive partitioning, and nominal logistic regression) with a variable IHC marker input. The histologic type was confirmed in 1521/1626 (93.5%) cases of the Canadian Ovarian Experimental Unified Resource and the Alberta Ovarian Tumor Type cohorts. The highest misclassification occurred in the endometrioid type, where most of the changes involved reclassification from endometrioid to high-grade serous carcinoma, which was additionally supported by mutational data and outcome. Using the reclassified histotype as the endpoint, a 4-marker prediction model correctly classified 88%, a 6-marker 91%, and an 8-marker 93% of the 1762 cases. This study provides statistically validated, inexpensive IHC algorithms, which have versatile applications in research, clinical practice, and clinical trials.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Ovarian Carcinoma Histotype: Strengths and Limitations of Integrating Morphology With Immunohistochemical Predictions.Int J Gynecol Pathol. 2019 Jul;38(4):353-362. doi: 10.1097/PGP.0000000000000530. Int J Gynecol Pathol. 2019. PMID: 29901523 Free PMC article.
-
High-grade Endometrioid Carcinoma of the Ovary: A Clinicopathologic Study of 30 Cases.Am J Surg Pathol. 2018 Apr;42(4):534-544. doi: 10.1097/PAS.0000000000001016. Am J Surg Pathol. 2018. PMID: 29309296
-
The histomorphology of Lynch syndrome-associated ovarian carcinomas: toward a subtype-specific screening strategy.Am J Surg Pathol. 2014 Sep;38(9):1173-81. doi: 10.1097/PAS.0000000000000298. Am J Surg Pathol. 2014. PMID: 25025451
-
Morphological subtypes of ovarian carcinoma: a review with emphasis on new developments and pathogenesis.Pathology. 2011 Aug;43(5):420-32. doi: 10.1097/PAT.0b013e328348a6e7. Pathology. 2011. PMID: 21716157 Review.
-
Ovarian Endometrioid Carcinoma Misdiagnosed as Mucinous Carcinoma: An Underrecognized Problem.Int J Gynecol Pathol. 2019 Nov;38(6):568-575. doi: 10.1097/PGP.0000000000000564. Int J Gynecol Pathol. 2019. PMID: 30480647 Review.
Cited by
-
Integrated molecular characterisation of endometrioid ovarian carcinoma identifies opportunities for stratification.NPJ Precis Oncol. 2021 Jun 2;5(1):47. doi: 10.1038/s41698-021-00187-y. NPJ Precis Oncol. 2021. PMID: 34079052 Free PMC article.
-
A Keratin 7 and E-Cadherin Signature Is Highly Predictive of Tubo-Ovarian High-Grade Serous Carcinoma Prognosis.Int J Mol Sci. 2021 May 18;22(10):5325. doi: 10.3390/ijms22105325. Int J Mol Sci. 2021. PMID: 34070214 Free PMC article.
-
From biobank and data silos into a data commons: convergence to support translational medicine.J Transl Med. 2021 Dec 4;19(1):493. doi: 10.1186/s12967-021-03147-z. J Transl Med. 2021. PMID: 34863191 Free PMC article.
-
SR-B1 and CD10 combined immunoprofile for differential diagnosis of metastatic clear cell renal cell carcinoma and clear cell carcinoma of the ovary.J Mol Histol. 2021 Jun;52(3):539-544. doi: 10.1007/s10735-021-09963-3. Epub 2021 Feb 19. J Mol Histol. 2021. PMID: 33608777 Free PMC article.
-
Ovarian Cancer Metastasis to the Larynx: A Case Report and Review of the Literature.Case Rep Surg. 2020 Aug 3;2020:1543129. doi: 10.1155/2020/1543129. eCollection 2020. Case Rep Surg. 2020. PMID: 32832186 Free PMC article.
References
-
- Köbel M, Kalloger SE, Huntsman DG, et al. Differences in tumor type in low-stage versus high-stage ovarian carcinomas. Int J Gynecol Pathol 2010;29:203–11. - PubMed
-
- Katsumata N, Yasuda M, Isonishi S, et al. Long-term results of dose-dense paclitaxel and carboplatin versus conventional paclitaxel and carboplatin for treatment of advanced epithelial ovarian, fallopian tube, or primary peritoneal cancer (JGOG 3016): a randomised, controlled, open-label trial. Lancet Oncol 2013;14:1020–6. - PubMed
-
- Kelemen LE, Köbel M. Mucinous carcinomas of the ovary and colorectum: different organ, same dilemma. Lancet Oncol 2011;12:1071–80. - PubMed
-
- Anglesio MS, Carey MS, Köbel M, et al. Clear cell carcinoma of the ovary: a report from the first Ovarian Clear Cell Symposium, June 24th, 2010. Gynecol Oncol 2011;121:407–15. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
