

Targeted Thromboelastographic (TEG) Blood Component and Pharmacologic Hemostatic Therapy in Traumatic and Acquired Coagulopathy
- PMID: 26960340
- PMCID: PMC5374842
- DOI: 10.2174/1389450117666160310153211
Targeted Thromboelastographic (TEG) Blood Component and Pharmacologic Hemostatic Therapy in Traumatic and Acquired Coagulopathy
Abstract
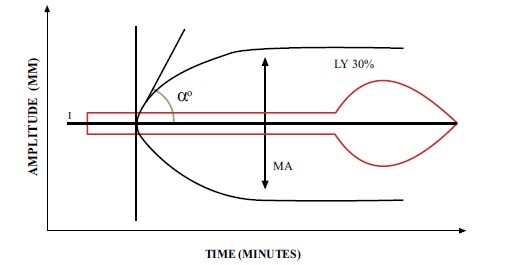
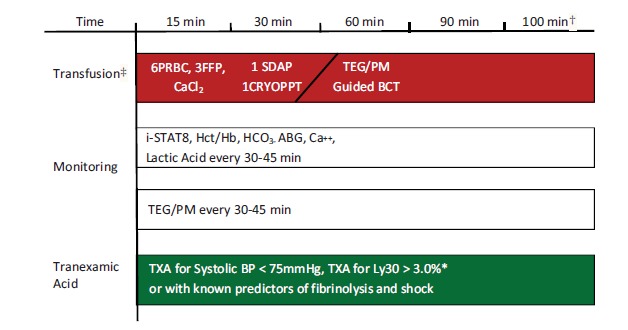
Trauma-induced coagulopathy (TIC) is a recently described condition which traditionally has been diagnosed by the common coagulation tests (CCTs) such as prothrombin time/international normalized ratio (PT/INR), activated partial thromboplastin time (aPTT), platelet count, and fibrinogen levels. The varying sensitivity and specificity of these CCTs have led trauma coagulation researchers and clinicians to use Viscoelastic Tests (VET) such as Thromboelastography (TEG) to provide Targeted Thromboelastographic Hemostatic and Adjunctive Therapy (TTHAT) in a goal directed fashion to those trauma patients in need of hemostatic resuscitation. This review describes the utility of VETs, in particular, TEG, to provide TTHAT in trauma and acquired non-trauma-induced coagulopathy.
Figures
Similar articles
-
Prehospital detection of traumatic coagulopathy.Transfusion. 2013 Jan;53 Suppl 1:48S-51S. doi: 10.1111/trf.12035. Transfusion. 2013. PMID: 23301972
-
Admission rapid thrombelastography can replace conventional coagulation tests in the emergency department: experience with 1974 consecutive trauma patients.Ann Surg. 2012 Sep;256(3):476-86. doi: 10.1097/SLA.0b013e3182658180. Ann Surg. 2012. PMID: 22868371
-
Viscoelastic testing in oncology patients (including for the diagnosis of fibrinolysis): Review of existing evidence, technology comparison, and clinical utility.Transfusion. 2020 Oct;60 Suppl 6:S86-S100. doi: 10.1111/trf.16102. Transfusion. 2020. PMID: 33089937 Review.
-
Goal-directed Hemostatic Resuscitation of Trauma-induced Coagulopathy: A Pragmatic Randomized Clinical Trial Comparing a Viscoelastic Assay to Conventional Coagulation Assays.Ann Surg. 2016 Jun;263(6):1051-9. doi: 10.1097/SLA.0000000000001608. Ann Surg. 2016. PMID: 26720428 Free PMC article. Clinical Trial.
-
Thromboelastography (TEG) and rotational thromboelastometry (ROTEM) for trauma induced coagulopathy in adult trauma patients with bleeding.Cochrane Database Syst Rev. 2015 Feb 16;2015(2):CD010438. doi: 10.1002/14651858.CD010438.pub2. Cochrane Database Syst Rev. 2015. PMID: 25686465 Free PMC article. Review.
Cited by
-
Markers of Futile Resuscitation in Traumatic Hemorrhage: A Review of the Evidence and a Proposal for Futility Time-Outs during Massive Transfusion.J Clin Med. 2024 Aug 9;13(16):4684. doi: 10.3390/jcm13164684. J Clin Med. 2024. PMID: 39200824 Free PMC article. Review.
-
Review of Thromboelastography (TEG): Medical and Surgical Applications.Ther Adv Pulm Crit Care Med. 2023 Dec 14;18:29768675231208426. doi: 10.1177/29768675231208426. eCollection 2023 Jul-Dec. Ther Adv Pulm Crit Care Med. 2023. PMID: 38107072 Free PMC article. Review.
-
Basic Principles of Rotational Thromboelastometry (ROTEM®) and the Role of ROTEM-Guided Fibrinogen Replacement Therapy in the Management of Coagulopathies.Diagnostics (Basel). 2023 Oct 16;13(20):3219. doi: 10.3390/diagnostics13203219. Diagnostics (Basel). 2023. PMID: 37892040 Free PMC article. Review.
-
Thromboelastography in the Perioperative Period: A Literature Review.Cureus. 2023 May 23;15(5):e39407. doi: 10.7759/cureus.39407. eCollection 2023 May. Cureus. 2023. PMID: 37362492 Free PMC article. Review.
-
Placental abruption at near-term and term gestations: pathophysiology, epidemiology, diagnosis, and management.Am J Obstet Gynecol. 2023 May;228(5S):S1313-S1329. doi: 10.1016/j.ajog.2022.06.059. Epub 2023 Mar 23. Am J Obstet Gynecol. 2023. PMID: 37164498 Free PMC article. Review.
References
-
- Frith D., Goslings J., Gaarder C., et al. Definition and drivers of acute traumatic coagulopathy: clinical and experimental investigations. J. Thromb. Haemost. 2010;8(9):1919–1925. - PubMed
-
- Brohi K., Singh J., Heron M., Coats T. Acute traumatic coagulopathy. J. Trauma. 2003;54(6):1127–1130. - PubMed
-
- Maegele M. Frequency, risk stratification and therapeutic management of acute post-traumatic coagulopathy. Vox Sang. 2009;97(1):39–49. - PubMed
-
- Maegele M., Lefering R., Yucel N., Tjardes T., Rixen D., Paffrath T. Early coagulopathy in multiple injury: an analysis from the german trauma registry on 8724 patients. Injury. 2007;38(3):298–304. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical