

Prevalence and characteristics of hypoxic hepatitis in the largest single-centre cohort of avian influenza A(H7N9) virus-infected patients with severe liver impairment in the intensive care unit
- PMID: 26733380
- PMCID: PMC4735056
- DOI: 10.1038/emi.2016.1
Prevalence and characteristics of hypoxic hepatitis in the largest single-centre cohort of avian influenza A(H7N9) virus-infected patients with severe liver impairment in the intensive care unit
Erratum in
-
Author Correction: Prevalence and characteristics of hypoxic hepatitis in the largest single-centre cohort of avian influenza A(H7N9) virus-infected patients with severe liver impairment in the intensive care unit.Emerg Microbes Infect. 2018 Mar 29;7(1):53. doi: 10.1038/s41426-018-0054-9. Emerg Microbes Infect. 2018. PMID: 29599488 Free PMC article.
Abstract
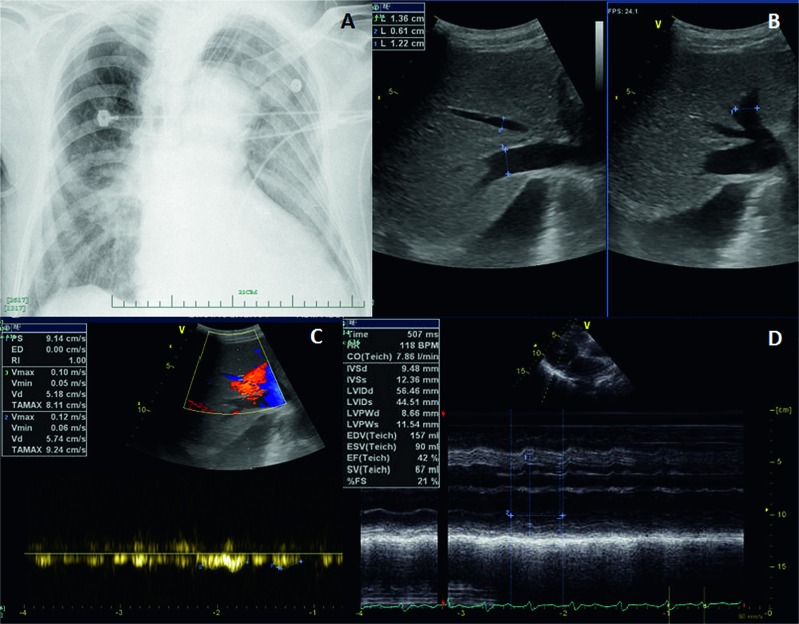
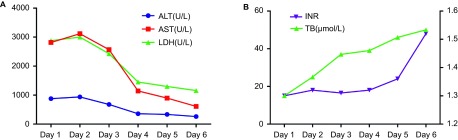
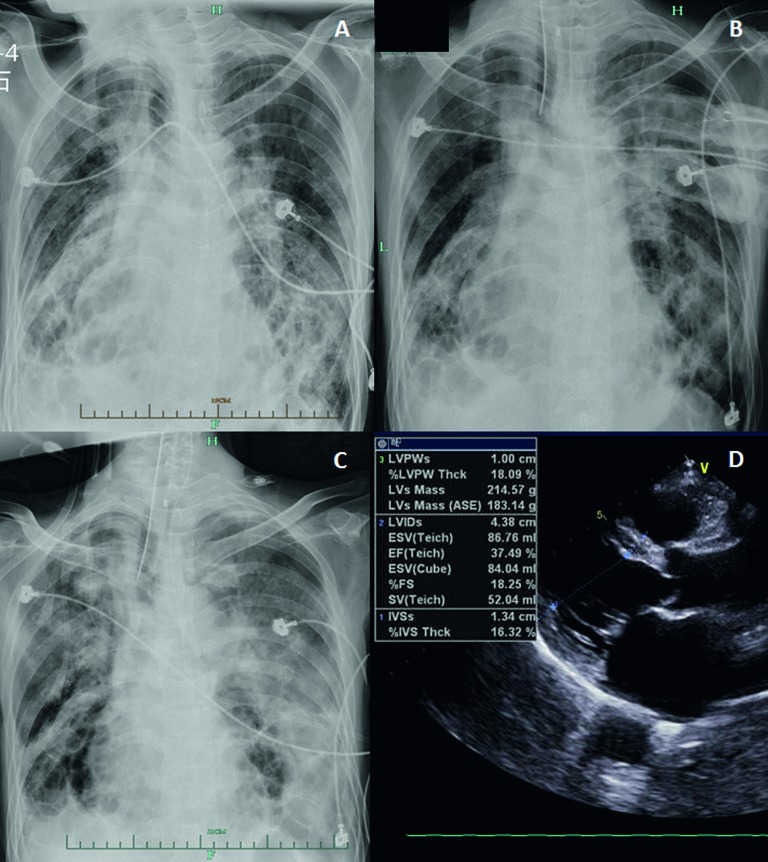
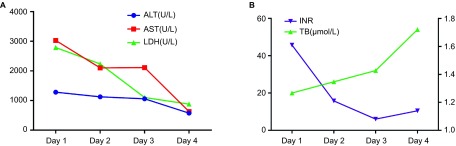
Avian influenza A(H7N9) virus (A(H7N9)) emerged in February 2013. Liver impairment of unknown cause is present in 29% of patients with A(H7N9) infection, some of whom experience severe liver injury. Hypoxic hepatitis (HH) is a type of acute severe liver injury characterized by an abrupt, massive increase in serum aminotransferases resulting from anoxic centrilobular necrosis of liver cells. In the intensive care unit (ICU), the prevalence of HH is ∼1%-2%. Here, we report a 1.8% (2/112) incidence of HH in the largest single-centre cohort of ICU patients with A(H7N9) infection. Both HH patients presented with multiple organ failure (MOF) involving respiratory, cardiac, circulatory and renal failure and had a history of chronic heart disease. On admission, severe liver impairment was found. Peak alanine aminotransferase (ALT) and aspartate aminotransferase (AST) values were 937 and 1281 U/L, and 3117 and 3029 U/L, respectively, in the two patients. Unfortunately, both patients died due to deterioration of MOF. A post-mortem biopsy in case 1 confirmed the presence of centrilobular necrosis of the liver, and real-time reverse transcription polymerase chain reaction of A(H7N9)-specific genes was negative, which excluded A(H7N9)-related hepatitis. The incidence of HH in A(H7N9) patients is similar to that in ICU patients with other aetiologies. It seems that patients with A(H7N9) infection and a history of chronic heart disease with a low left ventricular ejection fraction on admission are susceptible to HH, which presents as a marked elevation in ALT at the time of admission.
Figures

Similar articles
-
[A report of first fatal case of H10N8 avian influenza virus pneumonia in the world].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2014 Feb;26(2):120-2. doi: 10.3760/cma.j.issn.2095-4352.2014.02.013. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2014. PMID: 24524404 Chinese.
-
Novel avian-origin influenza A (H7N9) in critically ill patients in China*.Crit Care Med. 2015 Feb;43(2):339-45. doi: 10.1097/CCM.0000000000000695. Crit Care Med. 2015. PMID: 25365721
-
Muscle weakness associated with H7N9 infection: report of two cases.BMC Infect Dis. 2018 Dec 20;18(1):685. doi: 10.1186/s12879-018-3592-9. BMC Infect Dis. 2018. PMID: 30572825 Free PMC article.
-
Extracorporeal membrane oxygenation for avian influenza A (H7N9) patient with acute respiratory distress syndrome: a case report and short literature review.BMC Pulm Med. 2017 Feb 14;17(1):38. doi: 10.1186/s12890-017-0381-y. BMC Pulm Med. 2017. PMID: 28196469 Free PMC article. Review.
-
Successful management of refractory respiratory failure caused by avian influenza H7N9 and secondary organizing pneumonia: a case report and literature review.BMC Infect Dis. 2019 Jul 29;19(1):671. doi: 10.1186/s12879-019-4306-7. BMC Infect Dis. 2019. PMID: 31357937 Free PMC article. Review.
Cited by
-
Clinical indices and mortality of hospitalized avian influenza A (H7N9) patients in Guangdong, China.Chin Med J (Engl). 2019 Feb 5;132(3):302-310. doi: 10.1097/CM9.0000000000000043. Chin Med J (Engl). 2019. PMID: 30681496 Free PMC article.
-
Impacts of age and gender at the risk of underlying medical conditions and death in patients with avian influenza A (H7N9): a meta-analysis study.Ther Clin Risk Manag. 2018 Sep 6;14:1615-1626. doi: 10.2147/TCRM.S173834. eCollection 2018. Ther Clin Risk Manag. 2018. PMID: 30233197 Free PMC article.
-
Expression of inflammation-related genes in the lung of BALB/c mice response to H7N9 influenza A virus with different pathogenicity.Med Microbiol Immunol. 2016 Oct;205(5):501-9. doi: 10.1007/s00430-016-0466-x. Epub 2016 Jul 11. Med Microbiol Immunol. 2016. PMID: 27401907 Free PMC article.
-
Qing-Wen-Jie-Re Mixture Ameliorates Poly (I:C)-Induced Viral Pneumonia Through Regulating the Inflammatory Response and Serum Metabolism.Front Pharmacol. 2022 Jun 15;13:891851. doi: 10.3389/fphar.2022.891851. eCollection 2022. Front Pharmacol. 2022. PMID: 35784698 Free PMC article.
-
The viral distribution and pathological characteristics of BALB/c mice infected with highly pathogenic Influenza H7N9 virus.Virol J. 2021 Nov 29;18(1):237. doi: 10.1186/s12985-021-01709-7. Virol J. 2021. PMID: 34844617 Free PMC article.
References
-
- 1Gao R, Cao B, Hu Y et al. Human infection with a novel avian-origin influenza A (H7N9) virus. N Engl J Med 2013; 368: 1888–1897. - PubMed
-
- 2World Health Organization. WHO risk assessment of human infection with avian influenza A(H7N9) virus as of 23 February 2015. Geneva: WHO, 2015. Available at http://www.who.int/influenza/human_animal_interface/influenza_h7n9/RiskA... 2015. (accessed 8 August 2015).
-
- 5Zhang J, Zhao Y, Chen Y. Laboratory findings in patients with avian-origin influenza A (H7N9) virus infections. J Med Virol 2014; 86: 895–898. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical