

Epidemiology, Co-Infections, and Outcomes of Viral Pneumonia in Adults: An Observational Cohort Study
- PMID: 26683973
- PMCID: PMC5058945
- DOI: 10.1097/MD.0000000000002332
Epidemiology, Co-Infections, and Outcomes of Viral Pneumonia in Adults: An Observational Cohort Study
Abstract
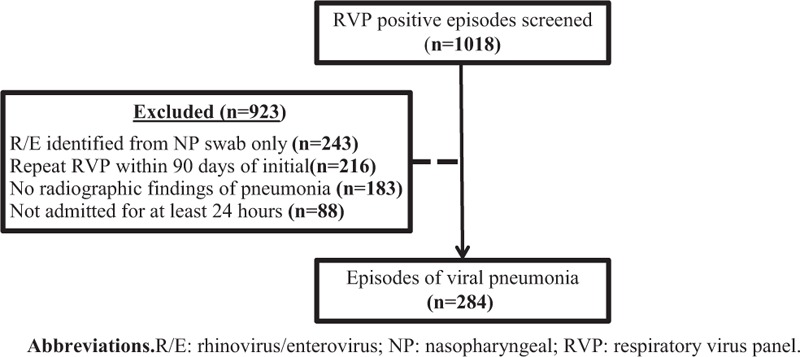
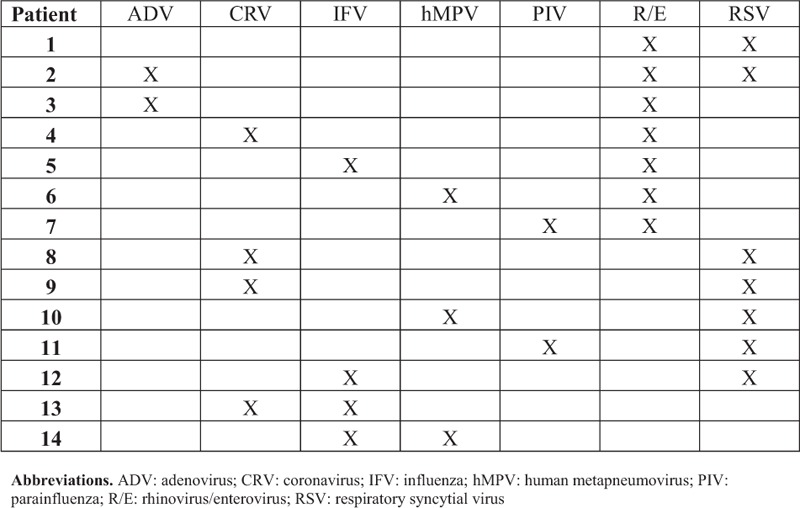
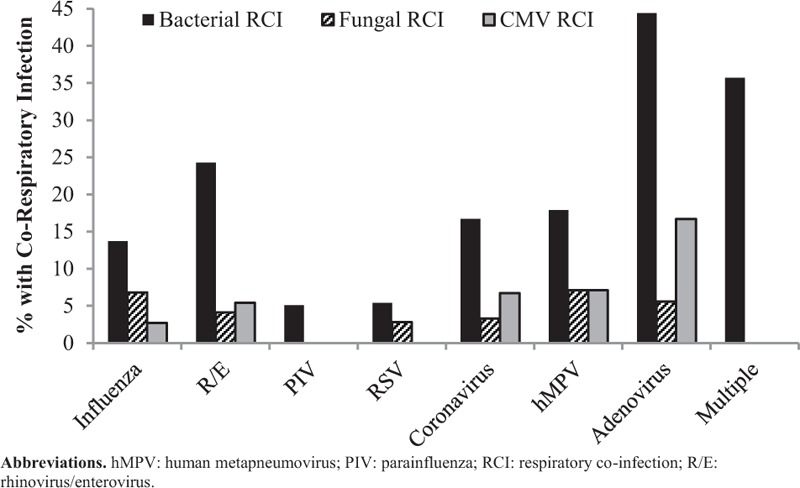
Advanced technologies using polymerase-chain reaction have allowed for increased recognition of viral respiratory infections including pneumonia. Co-infections have been described for several respiratory viruses, especially with influenza. Outcomes of viral pneumonia, including cases with co-infections, have not been well described. This was observational cohort study conducted to describe hospitalized patients with viral pneumonia including co-infections, clinical outcomes, and predictors of mortality. Patients admitted from March 2013 to November 2014 with a positive respiratory virus panel (RVP) and radiographic findings of pneumonia within 48 h of the index RVP were included. Co-respiratory infection (CRI) was defined as any organism identification from a respiratory specimen within 3 days of the index RVP. Predictors of in-hospital mortality on univariate analysis were evaluated in a multivariate model. Of 284 patients with viral pneumonia, a majority (51.8%) were immunocompromised. A total of 84 patients (29.6%) were found to have a CRI with 48 (57.6%) having a bacterial CRI. Viral CRI with HSV, CMV, or both occurred in 28 patients (33.3%). Fungal (16.7%) and other CRIs (7.1%) were less common. Many patients required mechanical ventilation (54%) and vasopressor support (36%). Overall in-hospital mortality was high (23.2%) and readmissions were common with several patients re-hospitalized within 30 (21.1%) and 90 days (36.7%) of discharge. Predictors of in-hospital mortality on multivariate regression included severity of illness factors, stem-cell transplant, and identification of multiple respiratory viruses. In conclusion, hospital mortality is high among adult patients with viral pneumonia and patients with multiple respiratory viruses identified may be at a higher risk.
Conflict of interest statement
All authors have declared no competing interests.
Figures
Similar articles
-
Impact of antibacterials on subsequent resistance and clinical outcomes in adult patients with viral pneumonia: an opportunity for stewardship.Crit Care. 2015 Nov 18;19:404. doi: 10.1186/s13054-015-1120-5. Crit Care. 2015. PMID: 26577540 Free PMC article.
-
Clinical characteristics and outcomes in hospitalized patients with respiratory viral co-infection during the 2009 H1N1 influenza pandemic.PLoS One. 2013 Apr 9;8(4):e60845. doi: 10.1371/journal.pone.0060845. Print 2013. PLoS One. 2013. PMID: 23585856 Free PMC article.
-
Bacterial and fungal coinfection among hospitalized patients with COVID-19: a retrospective cohort study in a UK secondary-care setting.Clin Microbiol Infect. 2020 Oct;26(10):1395-1399. doi: 10.1016/j.cmi.2020.06.025. Epub 2020 Jun 27. Clin Microbiol Infect. 2020. PMID: 32603803 Free PMC article.
-
Community-acquired bacterial co-infection predicts severity and mortality in influenza-associated pneumonia admitted patients.J Infect Chemother. 2019 Feb;25(2):129-136. doi: 10.1016/j.jiac.2018.10.014. Epub 2018 Nov 15. J Infect Chemother. 2019. PMID: 30448361
-
Pneumonia with bacterial and viral coinfection.Curr Opin Crit Care. 2017 Oct;23(5):385-390. doi: 10.1097/MCC.0000000000000435. Curr Opin Crit Care. 2017. PMID: 28777158 Review.
Cited by
-
Etiology, clinical, and epidemiological characteristics of severe respiratory infection in people living with HIV.Int J STD AIDS. 2020 Feb;31(2):100-108. doi: 10.1177/0956462419882587. Epub 2020 Jan 22. Int J STD AIDS. 2020. PMID: 31969059 Free PMC article.
-
Performance evaluation of direct fluorescent antibody, Focus Diagnostics Simplexa™ Flu A/B & RSV and multi-parameter customized respiratory Taqman® array card in immunocompromised patients.J Virol Methods. 2017 Jul;245:61-65. doi: 10.1016/j.jviromet.2017.03.013. Epub 2017 Mar 30. J Virol Methods. 2017. PMID: 28365410 Free PMC article.
-
Prospects on Repurposing a Live Attenuated Vaccine for the Control of Unrelated Infections.Front Immunol. 2022 May 16;13:877845. doi: 10.3389/fimmu.2022.877845. eCollection 2022. Front Immunol. 2022. PMID: 35651619 Free PMC article. Review.
-
Cardiovascular Disease and Coronavirus Disease 2019: Epidemiology, Management, and Prevention.Curr Epidemiol Rep. 2021;8(1):1-8. doi: 10.1007/s40471-020-00261-2. Epub 2021 Jan 2. Curr Epidemiol Rep. 2021. PMID: 33425654 Free PMC article. Review.
-
Role and Clinical Application of Metagenomic Next-Generation Sequencing in Immunocompromised Patients With Acute Respiratory Failure During Veno-Venous Extracorporeal Membrane Oxygenation.Front Cell Infect Microbiol. 2022 Aug 12;12:877205. doi: 10.3389/fcimb.2022.877205. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 36034706 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
