

Pharmacological targeting of chemokine (C-X-C motif) receptor 4 in porcine polytrauma and hemorrhage models
- PMID: 26683396
- PMCID: PMC4909050
- DOI: 10.1097/TA.0000000000000865
Pharmacological targeting of chemokine (C-X-C motif) receptor 4 in porcine polytrauma and hemorrhage models
Abstract
Background: Recent evidence suggests that chemokine receptor CXCR4 regulates vascular α1-adrenergic receptor function and that the noncognate CXCR4 agonist ubiquitin has therapeutic potential after trauma/hemorrhage. Pharmacologic properties of ubiquitin in large animal trauma models, however, are poorly characterized. Thus, the aims of the present study were to determine the effects of CXCR4 modulation on resuscitation requirements after polytrauma, to assess whether ubiquitin influences survival times after lethal polytrauma-hemorrhage, and to characterize its dose-effect profile in porcine models.
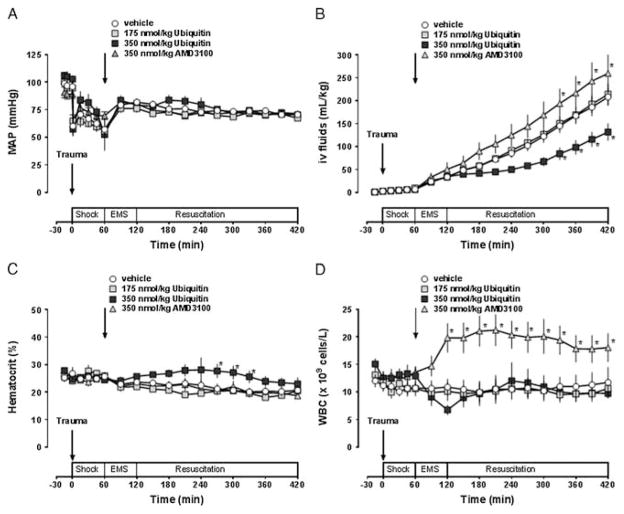
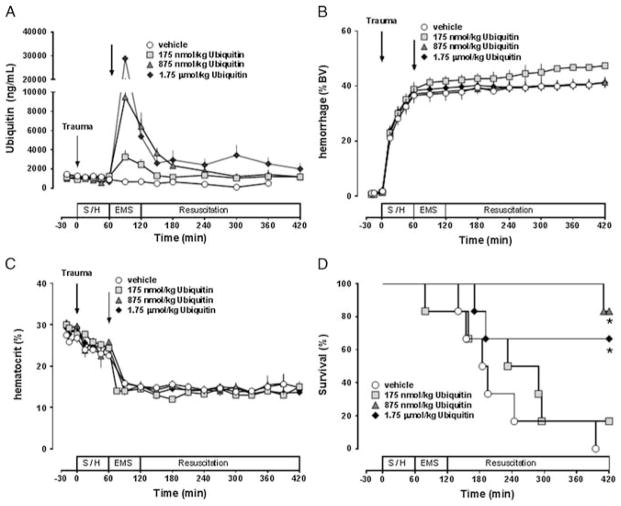
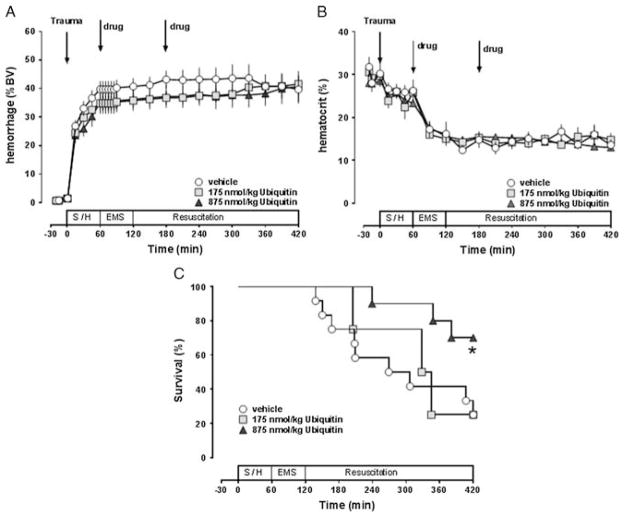
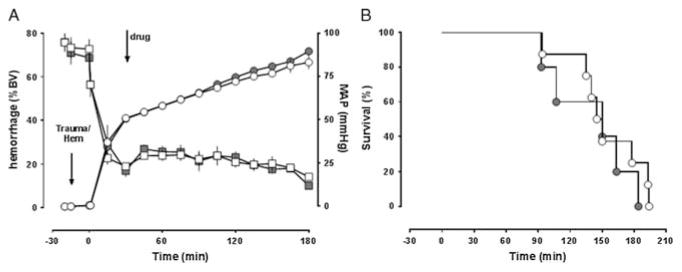
Methods: Anesthetized pigs underwent polytrauma (PT, femur fractures/lung contusion) alone (Series 1) or PT/hemorrhage (PT/H) to a mean arterial blood pressure of 30 mmHg with subsequent fluid resuscitation (Series 2 and 3) or 40% blood volume hemorrhage within 15 minutes followed by 2.5% blood volume hemorrhage every 15 minutes without fluid resuscitation (Series 4). In Series 1, ubiquitin (175 and 350 nmol/kg), AMD3100 (CXCR4 antagonist, 350 nmol/kg), or vehicle treatment 60 minutes after PT was performed. In Series 2, ubiquitin (175, 875, and 1,750 nmol/kg) or vehicle treatment 60 minutes after PT/H was performed. In Series 3, ubiquitin (175 and 875 nmol/kg) or vehicle treatment at 60 and 180 minutes after PT/H was performed. In Series 4, ubiquitin (875 nmol/kg) or vehicle treatment 30 minutes after hemorrhage was performed.
Results: In Series 1, resuscitation fluid requirements were significantly reduced by 40% with 350-nmol/kg ubiquitin and increased by 25% with AMD3100. In Series 2, median survival time was 190 minutes with vehicle, 260 minutes with 175-nmol/kg ubiquitin, and longer than 420 minutes with 875-nmol/kg and 1,750-nmol/kg ubiquitin (p < 0.05 vs. vehicle). In Series 3, median survival time was 288 minutes with vehicle and 336 minutes and longer than 420 minutes (p < 0.05 vs. vehicle) with 175-nmol/kg and 875-nmol/kg ubiquitin, respectively. In Series 4, median survival time was 147.5 minutes and 150 minutes with vehicle and ubiquitin, respectively (p > 0.05).
Conclusion: These findings further suggest CXCR4 as a drug target after PT/H. Ubiquitin treatment reduces resuscitation fluid requirements and provides survival benefits after PT/H. The pharmacological effects of ubiquitin treatment occur dose dependently.
Figures

Similar articles
-
Pharmacological modulation of C-X-C motif chemokine receptor 4 influences development of acute respiratory distress syndrome after lung ischaemia-reperfusion injury.Clin Exp Pharmacol Physiol. 2018 Jan;45(1):16-26. doi: 10.1111/1440-1681.12845. Epub 2017 Sep 20. Clin Exp Pharmacol Physiol. 2018. PMID: 28815665 Free PMC article.
-
Chemokine (C-X-C motif) receptor 4 regulates lung endothelial barrier permeability during resuscitation from hemorrhagic shock.Physiol Res. 2019 Aug 29;68(4):675-679. doi: 10.33549/physiolres.934105. Epub 2019 Jun 6. Physiol Res. 2019. PMID: 31177801 Free PMC article.
-
Initial assessment of the role of CXC chemokine receptor 4 after polytrauma.Mol Med. 2012 Sep 25;18(1):1056-66. doi: 10.2119/molmed.2011.00497. Mol Med. 2012. PMID: 22634721 Free PMC article.
-
Effects of exogenous ubiquitin in a polytrauma model with blunt chest trauma.Crit Care Med. 2012 Aug;40(8):2376-84. doi: 10.1097/CCM.0b013e3182514ed9. Crit Care Med. 2012. PMID: 22622399 Free PMC article.
-
Chemokine (C-X-C motif) receptor 4 and atypical chemokine receptor 3 regulate vascular α₁-adrenergic receptor function.Mol Med. 2014 Oct 13;20(1):435-47. doi: 10.2119/molmed.2014.00101. Mol Med. 2014. PMID: 25032954 Free PMC article.
Cited by
-
Pharmacological modulation of C-X-C motif chemokine receptor 4 influences development of acute respiratory distress syndrome after lung ischaemia-reperfusion injury.Clin Exp Pharmacol Physiol. 2018 Jan;45(1):16-26. doi: 10.1111/1440-1681.12845. Epub 2017 Sep 20. Clin Exp Pharmacol Physiol. 2018. PMID: 28815665 Free PMC article.
-
Natural and engineered chemokine (C-X-C motif) receptor 4 agonists prevent acute respiratory distress syndrome after lung ischemia-reperfusion injury and hemorrhage.Sci Rep. 2020 Jul 9;10(1):11359. doi: 10.1038/s41598-020-68425-0. Sci Rep. 2020. PMID: 32647374 Free PMC article.
-
Chemokine (C-X-C motif) receptor 4 regulates lung endothelial barrier permeability during resuscitation from hemorrhagic shock.Physiol Res. 2019 Aug 29;68(4):675-679. doi: 10.33549/physiolres.934105. Epub 2019 Jun 6. Physiol Res. 2019. PMID: 31177801 Free PMC article.
-
Identification and functional characterization of arginine vasopressin receptor 1A : atypical chemokine receptor 3 heteromers in vascular smooth muscle.Open Biol. 2018 Jan;8(1):170207. doi: 10.1098/rsob.170207. Open Biol. 2018. PMID: 29386406 Free PMC article.
-
α1-Adrenergic Receptors Function Within Hetero-Oligomeric Complexes With Atypical Chemokine Receptor 3 and Chemokine (C-X-C motif) Receptor 4 in Vascular Smooth Muscle Cells.J Am Heart Assoc. 2017 Aug 17;6(8):e006575. doi: 10.1161/JAHA.117.006575. J Am Heart Assoc. 2017. PMID: 28862946 Free PMC article.
References
-
- Heron M, Hoyert DL, Murphy SL, Xu J, Kochanek KD, Tejada-Vera B. Deaths: final data for 2006. Natl Vital Stat Rep. 2009;57(14):1–134. - PubMed
-
- Kauvar DS, Lefering R, Wade CE. Impact of hemorrhage on trauma outcome: an overview of epidemiology, clinical presentations, and therapeutic considerations. J Trauma. 2006;60(6 Suppl):S3–S11. - PubMed
-
- Cohn SM, Blackbourne LH, Landry DW, Proctor KG, Walley KR, Wenzel V. San Antonio Vasopressin in Shock Symposium report. Resuscitation. 2010;81(11):1473–1475. - PubMed
-
- Anand T, Skinner R. Arginine vasopressin: the future of pressure-support resuscitation in hemorrhagic shock. J Surg Res. 2012;178(1):321–329. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
