

Sevelamer Versus Calcium-Based Binders for Treatment of Hyperphosphatemia in CKD: A Meta-Analysis of Randomized Controlled Trials
- PMID: 26668024
- PMCID: PMC4741042
- DOI: 10.2215/CJN.06800615
Sevelamer Versus Calcium-Based Binders for Treatment of Hyperphosphatemia in CKD: A Meta-Analysis of Randomized Controlled Trials
Abstract
Background and objectives: People with CKD stages 3-5 and on dialysis (5D) have dramatically increased mortality, which has been associated with hyperphosphatemia in many studies. Oral phosphate binders are commonly prescribed to lower serum phosphate. We conducted an updated meta-analysis of the noncalcium-based binder (non-CBB) sevelamer versus CBBs in CKD stages 3-5D.
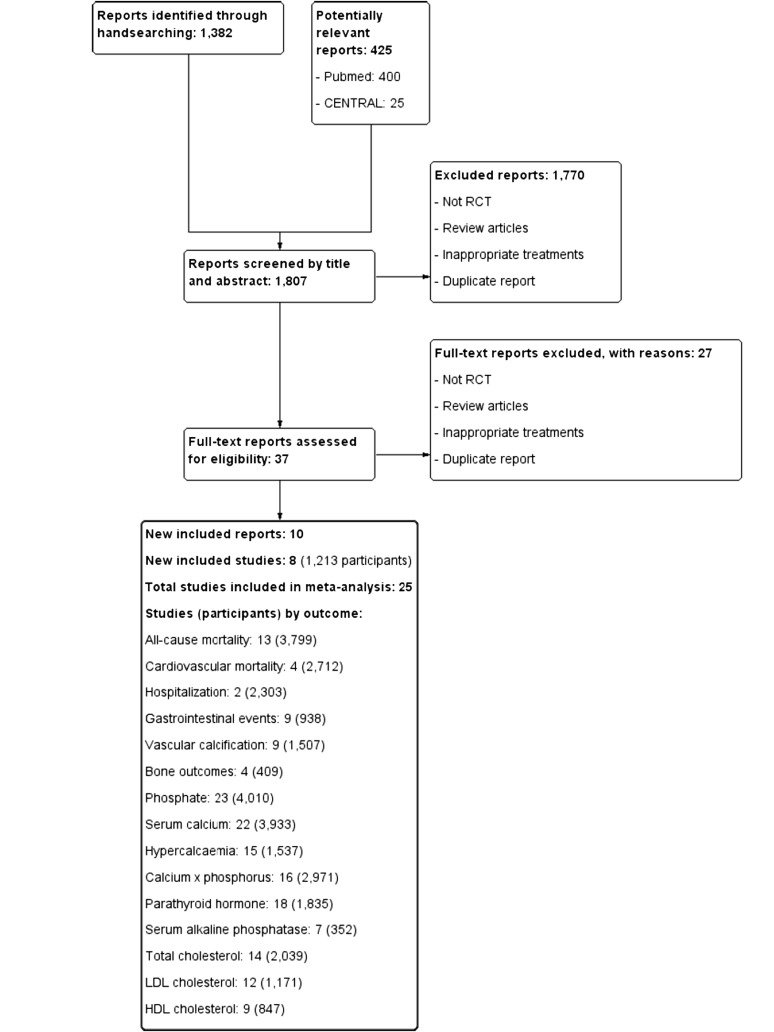
Design, setting, participants, & measurements: Randomized, controlled trials comparing sevelamer with CBBs were identified through MEDLINE and the Cochrane Central Register of Controlled Trials. Patient-level outcomes included all-cause mortality, cardiovascular events and mortality, hospitalization, and adverse effects. Intermediate outcomes included vascular calcification and bone changes. Biochemical outcomes included serum phosphate, calcium, parathyroid hormone, lipids, and hypercalcemia. We conducted and reported this review according to Cochrane guidelines.
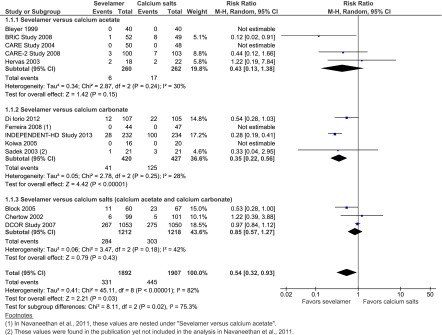
Results: We included 25 studies to March 31, 2015 with 4770 participants (88% on hemodialysis). Patients receiving sevelamer had lower all-cause mortality (risk ratio [RR], 0.54; 95% confidence interval [95% CI], 0.32 to 0.93), no statistically significant difference in cardiovascular mortality (n=2712; RR, 0.33; 95% CI, 0.07 to 1.64), and an increase in combined gastrointestinal events of borderline statistical significance (n=384; RR, 1.42; 95% CI, 0.97 to 2.08). For biochemical outcomes, patients receiving sevelamer had lower total serum cholesterol (mean difference [MD], -20.2 mg/dl; 95% CI, -25.9 to -14.5 mg/dl), LDL-cholesterol (MD, -21.6 mg/dl; 95% CI, -27.9 to -15.4 mg/dl), and calcium (MD, -0.4 mg/dl; 95% CI, -0.6 to -0.2 mg/dl) and a reduced risk of hypercalcemia (RR, 0.30; 95% CI, 0.19 to 0.48). End of treatment intact parathyroid hormone was significantly higher for sevelamer (MD, 32.9 pg/ml; 95% CI, 0.1 to 65.7 pg/ml). Serum phosphate values showed no significant differences.
Conclusions: Patients with CKD stages 3-5D using sevelamer have lower all-cause mortality compared with those using CBBs. Because of a lack of placebo-controlled studies, questions remain regarding phosphate binder benefits for patients with CKD stages 3-5 and not on dialysis.
Keywords: calcium; chronic kidney disease; hospitalization; humans; meta-analysis; mortality; phosphate binders; randomized controlled trials as topic; sevelamer.
Copyright © 2016 by the American Society of Nephrology.
Figures
Similar articles
-
Benefits and harms of phosphate binders in CKD: a systematic review of randomized controlled trials.Am J Kidney Dis. 2009 Oct;54(4):619-37. doi: 10.1053/j.ajkd.2009.06.004. Epub 2009 Aug 18. Am J Kidney Dis. 2009. PMID: 19692157 Review.
-
Phosphate binders for preventing and treating chronic kidney disease-mineral and bone disorder (CKD-MBD).Cochrane Database Syst Rev. 2018 Aug 22;8(8):CD006023. doi: 10.1002/14651858.CD006023.pub3. Cochrane Database Syst Rev. 2018. PMID: 30132304 Free PMC article.
-
The efficacy and safety of sevelamer and lanthanum versus calcium-containing and iron-based binders in treating hyperphosphatemia in patients with chronic kidney disease: a systematic review and meta-analysis.Nephrol Dial Transplant. 2017 Jan 1;32(1):111-125. doi: 10.1093/ndt/gfw312. Nephrol Dial Transplant. 2017. PMID: 27651467 Review.
-
Initiation of Sevelamer and Mortality among Hemodialysis Patients Treated with Calcium-Based Phosphate Binders.Clin J Am Soc Nephrol. 2017 Sep 7;12(9):1489-1497. doi: 10.2215/CJN.13091216. Epub 2017 Jul 19. Clin J Am Soc Nephrol. 2017. PMID: 28724618 Free PMC article.
-
Phosphate binders for preventing and treating bone disease in chronic kidney disease patients.Cochrane Database Syst Rev. 2011 Feb 16;(2):CD006023. doi: 10.1002/14651858.CD006023.pub2. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2018 Aug 22;8:CD006023. doi: 10.1002/14651858.CD006023.pub3 PMID: 21328279 Updated. Review.
Cited by
-
Clustering phosphate and iron-related markers and prognosis in dialysis patients.Clin Kidney J. 2021 Oct 14;15(2):328-337. doi: 10.1093/ckj/sfab207. eCollection 2022 Feb. Clin Kidney J. 2021. PMID: 35145647 Free PMC article.
-
Coronary Artery Disease in Chronic Kidney Disease: Need for a Heart-Kidney Team-Based Approach.Eur Cardiol. 2021 Dec 7;16:e48. doi: 10.15420/ecr.2021.30. eCollection 2021 Feb. Eur Cardiol. 2021. PMID: 34950244 Free PMC article. Review.
-
Management of Secondary Hyperparathyroidism in Chronic Kidney Disease: A Focus on the Elderly.Drugs Aging. 2019 Oct;36(10):885-895. doi: 10.1007/s40266-019-00696-3. Drugs Aging. 2019. PMID: 31304565 Review.
-
The efficacy and safety of cuttlebone for lowering serum phosphate in patients with end-stage renal disease: a meta-analysis of randomized controlled trials.Front Pharmacol. 2023 Jul 24;14:1206366. doi: 10.3389/fphar.2023.1206366. eCollection 2023. Front Pharmacol. 2023. PMID: 37554990 Free PMC article.
-
Phosphate Binders and Nonphosphate Effects in the Gastrointestinal Tract.J Ren Nutr. 2020 Jan;30(1):4-10. doi: 10.1053/j.jrn.2019.01.004. Epub 2019 Mar 4. J Ren Nutr. 2020. PMID: 30846238 Free PMC article. Review.
References
-
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Work Group : KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl 76[113]: S1–S130, 2009 - PubMed
-
- Lopes AA, Tong L, Thumma J, Li Y, Fuller DS, Morgenstern H, Bommer J, Kerr PG, Tentori F, Akiba T, Gillespie BW, Robinson BM, Port FK, Pisoni RL: Phosphate binder use and mortality among hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study (DOPPS): Evaluation of possible confounding by nutritional status. Am J Kidney Dis 60: 90–101, 2012 - PMC - PubMed
-
- Cannata-Andía JB, Fernández-Martín JL, Locatelli F, London G, Gorriz JL, Floege J, Ketteler M, Ferreira A, Covic A, Rutkowski B, Memmos D, Bos WJ, Teplan V, Nagy J, Tielemans C, Verbeelen D, Goldsmith D, Kramar R, Martin PY, Wüthrich RP, Pavlovic D, Benedik M, Sánchez JE, Martínez-Camblor P, Naves-Díaz M, Carrero JJ, Zoccali C: Use of phosphate-binding agents is associated with a lower risk of mortality. Kidney Int 84: 998–1008, 2013 - PubMed
-
- Tonelli M, Pannu N, Manns B: Oral phosphate binders in patients with kidney failure. N Engl J Med 362: 1312–1324, 2010 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
