

A Time-Stratified Case-Crossover Study of Ambient Ozone Exposure and Emergency Department Visits for Specific Respiratory Diagnoses in California (2005-2008)
- PMID: 26647366
- PMCID: PMC4892911
- DOI: 10.1289/ehp.1409495
A Time-Stratified Case-Crossover Study of Ambient Ozone Exposure and Emergency Department Visits for Specific Respiratory Diagnoses in California (2005-2008)
Abstract
Background: Studies have explored ozone's connection to asthma and total respiratory emergency department visits (EDVs) but have neglected other specific respiratory diagnoses despite hypotheses relating ozone to respiratory infections and allergic responses.
Objective: We examined relationships between ozone and EDVs for respiratory visits, including specifically acute respiratory infections (ARI), asthma, pneumonia, chronic obstructive pulmonary disease (COPD), and upper respiratory tract inflammation (URTI).
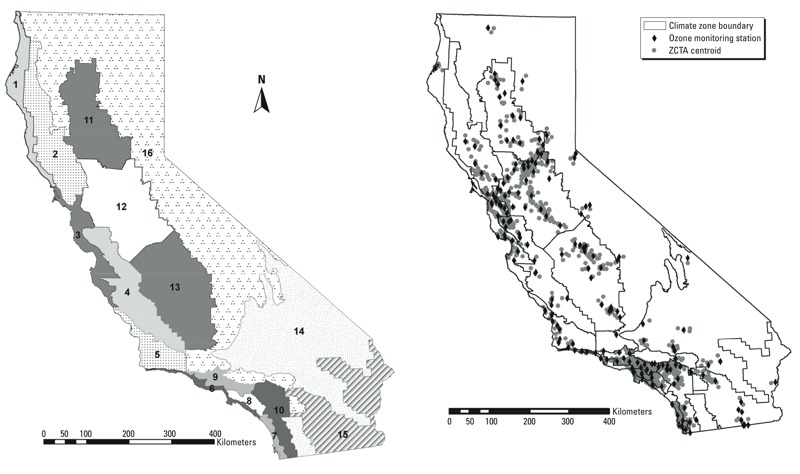
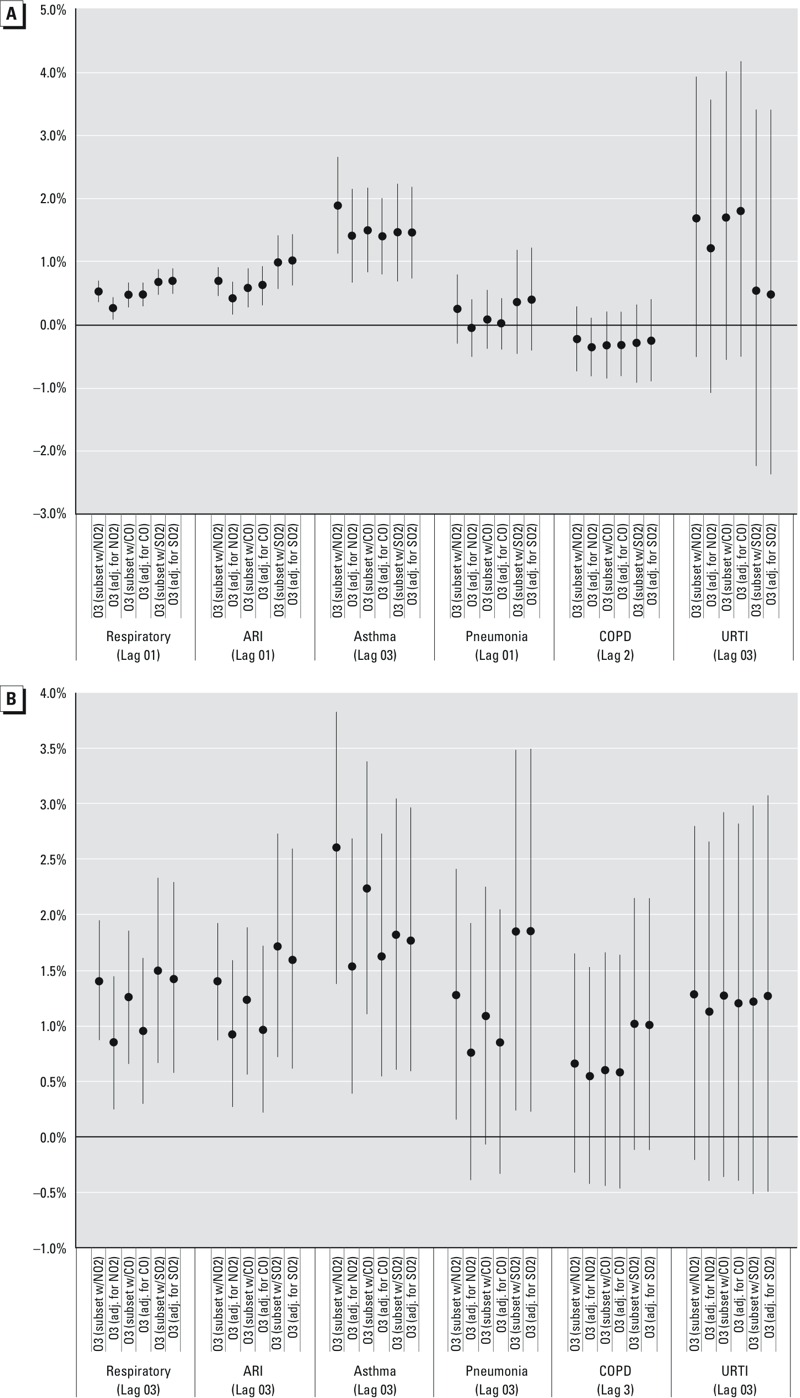
Methods: We conducted a multi-site time-stratified case-crossover study of ozone exposures for approximately 3.7 million respiratory EDVs from 2005 through 2008 among California residents living within 20 km of an ozone monitor. Conditional logistic regression was used to estimate associations by climate zone. Random effects meta-analysis was then applied to estimate pooled excess risks (ER). Effect modification by season, distance from the monitor and individual demographic characteristics (i.e., age, race/ethnicity, sex, and payment method), and confounding by other gaseous air pollutants were also investigated. Meta-regression was utilized to explore how climate zone-level meteorological, demographic, and regional differences influenced estimates.
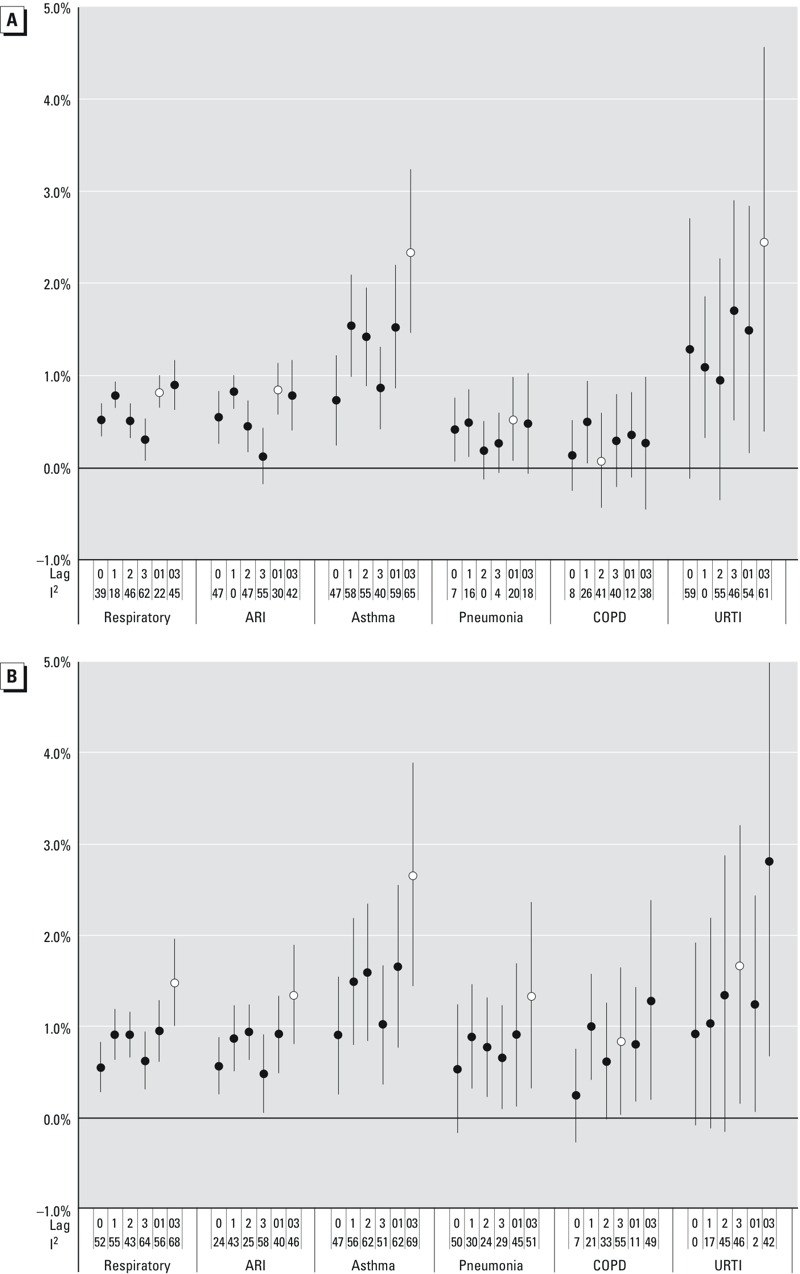
Results: We observed ozone-associated increases in all respiratory, asthma, and ARI visits, which were slightly larger in the warm season [asthma ER per 10-ppb increase in mean of same and previous 3 days ozone exposure (lag03) = 2.7%, 95% CI: 1.5, 3.9; ARI ERlag03 = 1.4%, 95% CI: 0.8, 1.9]. EDVs for pneumonia, COPD, and URTI were also significantly associated with ozone exposure over the whole year, but typically more consistently so during the warm season.
Conclusions: Short-term ozone exposures among California residents living near an ozone monitor were positively associated with EDVs for asthma, ARI, pneumonia, COPD, and URTI from 2005 through 2008. Those associations were typically larger and more consistent during the warm season. Our findings suggest that these outcomes should be considered when evaluating the potential health benefits of reducing ozone concentrations.
Citation: Malig BJ, Pearson DL, Chang YB, Broadwin R, Basu R, Green RS, Ostro B. 2016. A time-stratified case-crossover study of ambient ozone exposure and emergency department visits for specific respiratory diagnoses in California (2005-2008). Environ Health Perspect 124:745-753; http://dx.doi.org/10.1289/ehp.1409495.
Conflict of interest statement
The authors declare they have no actual or potential competing financial interests.
Figures

Similar articles
-
Multicity study of air pollution and mortality in Latin America (the ESCALA study).Res Rep Health Eff Inst. 2012 Oct;(171):5-86. Res Rep Health Eff Inst. 2012. PMID: 23311234
-
Effects of short-term exposure to air pollution on hospital admissions of young children for acute lower respiratory infections in Ho Chi Minh City, Vietnam.Res Rep Health Eff Inst. 2012 Jun;(169):5-72; discussion 73-83. Res Rep Health Eff Inst. 2012. PMID: 22849236
-
Pediatric Emergency Visits and Short-Term Changes in PM2.5 Concentrations in the U.S. State of Georgia.Environ Health Perspect. 2016 May;124(5):690-6. doi: 10.1289/ehp.1509856. Epub 2015 Oct 9. Environ Health Perspect. 2016. PMID: 26452298 Free PMC article.
-
Health effects of outdoor air pollution. Committee of the Environmental and Occupational Health Assembly of the American Thoracic Society.Am J Respir Crit Care Med. 1996 Jan;153(1):3-50. doi: 10.1164/ajrccm.153.1.8542133. Am J Respir Crit Care Med. 1996. PMID: 8542133 Review.
-
Effects of ambient ozone concentrations with different averaging times on asthma exacerbations: A meta-analysis.Sci Total Environ. 2019 Nov 15;691:549-561. doi: 10.1016/j.scitotenv.2019.06.382. Epub 2019 Jul 4. Sci Total Environ. 2019. PMID: 31325855 Review.
Cited by
-
Ozone and childhood respiratory health: A primer for US pediatric providers and a call for a more protective standard.Pediatr Pulmonol. 2023 May;58(5):1355-1366. doi: 10.1002/ppul.26368. Epub 2023 Mar 8. Pediatr Pulmonol. 2023. PMID: 36815617 Free PMC article. Review.
-
A multicity study of air pollution and cardiorespiratory emergency department visits: Comparing approaches for combining estimates across cities.Environ Int. 2018 Nov;120:312-320. doi: 10.1016/j.envint.2018.07.033. Epub 2018 Aug 11. Environ Int. 2018. PMID: 30107292 Free PMC article.
-
Long-term exposure to NO2 and O3 and all-cause and respiratory mortality: A systematic review and meta-analysis.Environ Int. 2020 Nov;144:105998. doi: 10.1016/j.envint.2020.105998. Epub 2020 Oct 5. Environ Int. 2020. PMID: 33032072 Free PMC article.
-
Updated Global Estimates of Respiratory Mortality in Adults ≥30Years of Age Attributable to Long-Term Ozone Exposure.Environ Health Perspect. 2017 Aug 28;125(8):087021. doi: 10.1289/EHP1390. Environ Health Perspect. 2017. PMID: 28858826 Free PMC article.
-
Spatiotemporal assessment of health burden and economic losses attributable to short-term exposure to ground-level ozone during 2015-2018 in China.BMC Public Health. 2021 Jun 5;21(1):1069. doi: 10.1186/s12889-021-10751-7. BMC Public Health. 2021. PMID: 34090376 Free PMC article.
References
-
- Arbex MA, de Souza Conceição GM, Cendon SP, Arbex FF, Lopes AC, Moysés EP, et al. Urban air pollution and chronic obstructive pulmonary disease-related emergency department visits. J Epidemiol Community Health. 2009;63:777–783. - PubMed
-
- Ayres JG, Borm P, Cassee FR, Castranova V, Donaldson K, Ghio A, et al. Evaluating the toxicity of airborne particulate matter and nanoparticles by measuring oxidative stress potential—a workshop report and consensus statement. Inhal Toxicol. 2008;20:75–99. - PubMed
-
- Basu R, Feng WY, Ostro BD. Characterizing temperature and mortality in nine California counties. Epidemiology. 2008;19:138–145. - PubMed
-
- Bell ML. The use of ambient air quality modeling to estimate individual and population exposure for human health research: a case study of ozone in the Northern Georgia Region of the United States. Environ Int. 2006;32:586–593. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
