

Clustering symptoms of non-severe malaria in semi-immune Amazonian patients
- PMID: 26500831
- PMCID: PMC4614890
- DOI: 10.7717/peerj.1325
Clustering symptoms of non-severe malaria in semi-immune Amazonian patients
Abstract
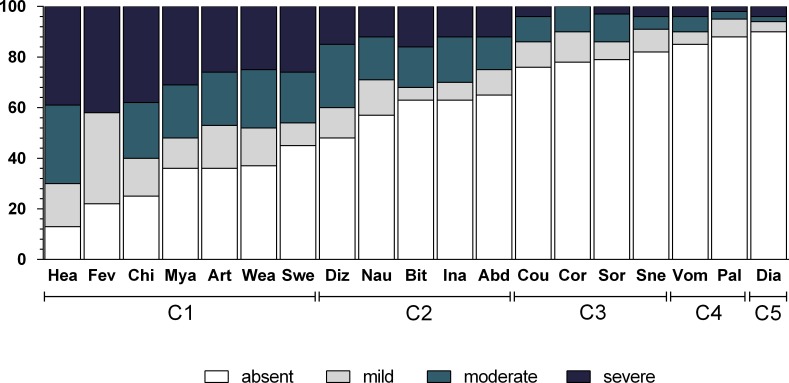
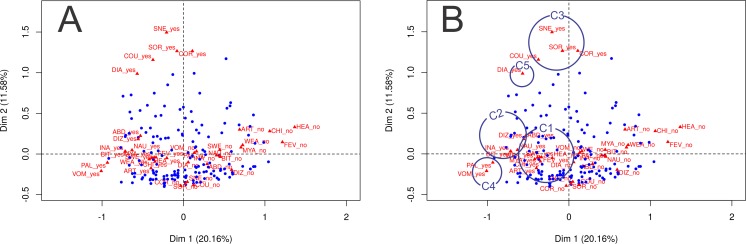
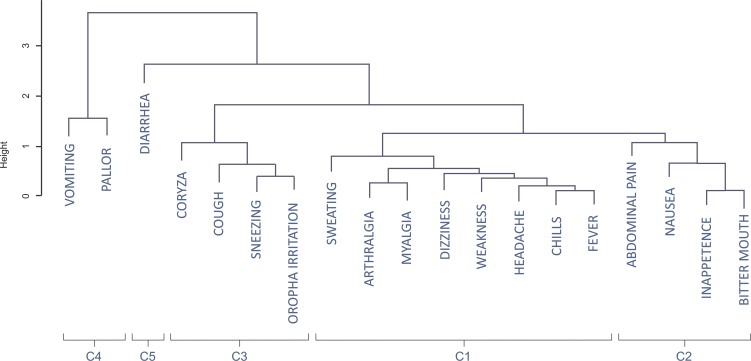
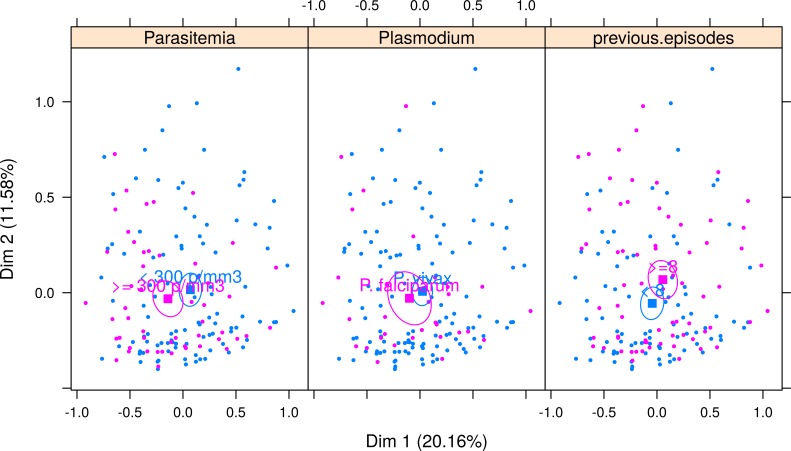
Malaria is a disease that generates a broad spectrum of clinical features. The purpose of this study was to evaluate the clinical spectrum of malaria in semi-immune populations. Patients were recruited in Mâncio Lima, a city situated in the Brazilian Amazon region. The study included 171 malaria cases, which were diagnosed via the use of a thick blood smear and confirmed by molecular methods. A questionnaire addressing 19 common symptoms was administered to all patients. Multiple correspondence analysis and hierarchical cluster analysis were performed to identify clusters of symptoms, and logistic regression was used to identify factors associated with the occurrence of symptoms. The cluster analysis revealed five groups of symptoms: the first cluster, which included algic- and fever-related symptoms, occurred in up to 95.3% of the cases. The second cluster, which comprised gastric symptoms (nausea, abdominal pain, inappetence, and bitter mouth), occurred in frequencies that ranged between 35.1% and 42.7%, and at least one of these symptoms was observed in 71.9% of the subjects. All respiratory symptoms were clustered and occurred in 42.7% of the malaria cases, and diarrhea occurred in 9.9% of the cases. Symptoms constituting the fifth cluster were vomiting and pallor, with a 14.6% and 11.7% of prevalence, respectively. A higher parasitemia count (more than 300 parasites/mm(3)) was associated with the presence of fever, vomiting, dizziness, and weakness (P < 0.05). Arthralgia and myalgia were associated with patients over the age of 14 years (P < 0.001). Having experienced at least eight malaria episodes prior to the study was associated with a decreased risk of chills and fever and an increased risk of sore throat (P < 0.05). None of the symptoms showed an association with gender or with species of Plasmodium. The clinical spectrum of malaria in semi-immune individuals can have a broad range of symptoms, the frequency and intensity of which are associated with age, past exposure to malaria, and parasitemia. Understanding the full spectrum of nonsevere malaria is important in endemic areas to guide both passive and active case detection, for the diagnosis of malaria in travelers returning to non-endemic areas, and for the development of vaccines aimed to decrease symptom severity.
Keywords: Amazon; Clustering; Malaria; Symtoms.
Conflict of interest statement
The authors declare there are no competing interests.
Figures

Similar articles
-
Malaria and other febrile diseases among travellers: the experience of a reference centre located outside the Brazilian Amazon Region.Malar J. 2016 May 26;15(1):294. doi: 10.1186/s12936-016-1347-x. Malar J. 2016. PMID: 27230739 Free PMC article.
-
Clinical spectrum of uncomplicated malaria in semi-immune Amazonians: beyond the " symptomatic " vs " asymptomatic " dichotomy.Mem Inst Oswaldo Cruz. 2007 Jun;102(3):341-7. doi: 10.1590/s0074-02762007005000051. Mem Inst Oswaldo Cruz. 2007. PMID: 17568940
-
Side Effects of Chloroquine and Primaquine and Symptom Reduction in Malaria Endemic Area (Mâncio Lima, Acre, Brazil).Interdiscip Perspect Infect Dis. 2015;2015:346853. doi: 10.1155/2015/346853. Epub 2015 Aug 18. Interdiscip Perspect Infect Dis. 2015. PMID: 26357512 Free PMC article.
-
Plasmodium knowlesi in travellers, update 2014.Int J Infect Dis. 2014 May;22:55-64. doi: 10.1016/j.ijid.2013.12.016. Epub 2014 Mar 12. Int J Infect Dis. 2014. PMID: 24631521 Review.
-
Diagnosis and Treatment of the Febrile Child.In: Black RE, Laxminarayan R, Temmerman M, Walker N, editors. Reproductive, Maternal, Newborn, and Child Health: Disease Control Priorities, Third Edition (Volume 2). Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2016 Apr 5. Chapter 8. In: Black RE, Laxminarayan R, Temmerman M, Walker N, editors. Reproductive, Maternal, Newborn, and Child Health: Disease Control Priorities, Third Edition (Volume 2). Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2016 Apr 5. Chapter 8. PMID: 27227231 Free Books & Documents. Review.
Cited by
-
Confounding influences of malnutrition and Plasmodium falciparum and Schistosoma haematobium infections on haematological parameters in school children in Muyuka, Cameroon.BMC Infect Dis. 2021 May 25;21(1):477. doi: 10.1186/s12879-021-06201-9. BMC Infect Dis. 2021. PMID: 34034666 Free PMC article.
-
Socioeconomic and demographic characterization of an endemic malaria region in Brazil by multiple correspondence analysis.Malar J. 2017 Oct 2;16(1):397. doi: 10.1186/s12936-017-2045-z. Malar J. 2017. PMID: 28969634 Free PMC article.
-
Does Malaria Cause Diarrhoea? A Systematic Review.Front Med (Lausanne). 2020 Nov 19;7:589379. doi: 10.3389/fmed.2020.589379. eCollection 2020. Front Med (Lausanne). 2020. PMID: 33330549 Free PMC article.
-
The Nociceptive and Inflammatory Responses Induced by the Ehrlich Solid Tumor Are Changed in Mice Healed of Plasmodium berghei Strain ANKA Infection after Chloroquine Treatment.J Parasitol Res. 2024 May 14;2024:3771926. doi: 10.1155/2024/3771926. eCollection 2024. J Parasitol Res. 2024. PMID: 38774541 Free PMC article.
-
Malaria and other febrile diseases among travellers: the experience of a reference centre located outside the Brazilian Amazon Region.Malar J. 2016 May 26;15(1):294. doi: 10.1186/s12936-016-1347-x. Malar J. 2016. PMID: 27230739 Free PMC article.
References
-
- Acre . State program of ecological-economical assessment of state of Acre. Phase II: synthesis document. 2nd edition. Rio Branco: Secretaria de Estado de Meio Ambiente e Recursos Naturais; 2010. Governo do Estado do Acre. 358 p.
-
- Anstey NM, Jacups SP, Cain T, Pearson T, Ziesing PJ, Fisher DA, Currie bJ, Marks PJ, Maguire GP. Pulmonary manifestations of uncomplicated falciparum and vivax malaria: cough, small airways obstruction, impaired gas transfer, and increased pulmonary phagocytic activity. Journal of Infectios Diseases. 2002;185:1326–1334. doi: 10.1086/339885. - DOI - PubMed
-
- Arévalo-Herrera M, Forero-Peña DA, Rubiano K, Gómez-Hincapie J, Martínez NL, Lopez-Perez M, Castellanos A, Céspedes N, Palacios R, Oñate JM, Herrera S. Plasmodium vivax sporozoite challenge in malaria-naïve and semi-immune Colombian volunteers. PLoS ONE. 2014;9(6):e1325. doi: 10.1371/journal.pone.0099754. - DOI - PMC - PubMed
-
- Carvalho MS, Struchiner CJ. Análise de correspondência: uma aplicação do método à avaliação de serviços de vacinação. Cadernos de Saúde Pública. 1992;8:287–301. doi: 10.1590/S0102-311X1992000300008. - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
