

Risk Factors for Central Lymph Node Metastasis in CN0 Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis
- PMID: 26431346
- PMCID: PMC4592212
- DOI: 10.1371/journal.pone.0139021
Risk Factors for Central Lymph Node Metastasis in CN0 Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis
Abstract
Background: Central lymph node metastasis (CLNM) is common in papillary thyroid carcinoma (PTC). Prophylactic central lymph node dissection (PCLND) for patients with clinically negative central compartment lymph nodes (CN0) remains controversial. The phrase "clinically negative" is used to indicate that patients exhibited no clinical evidence of CLNM by ultrasonography (US) or computerized tomography (CT) preoperatively. In this study, we analyze the risk factors for CLNM in CN0 patients.
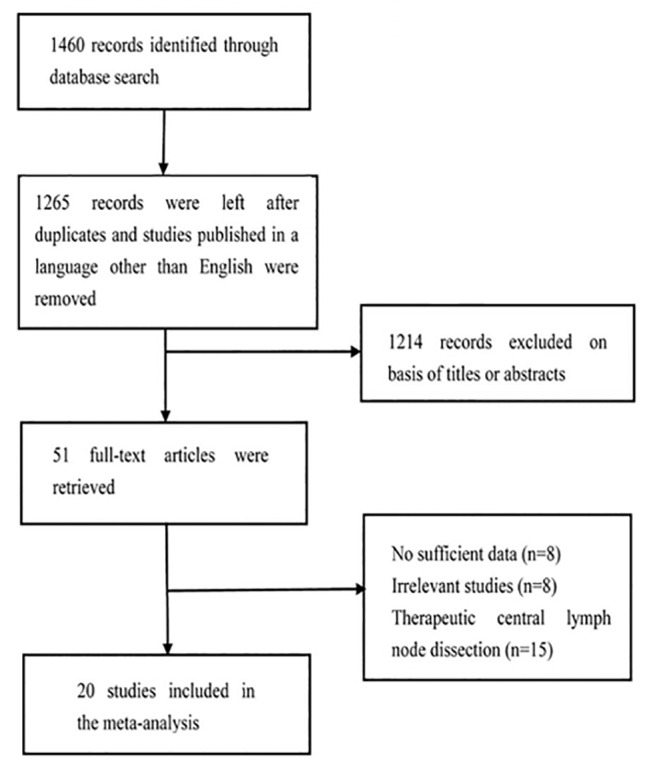
Methods: The PUBMED and SCIE databases were systematically searched for works published through January 31, 2015. All of the patients included in this study underwent thyroidectomy+PCLND. Revman 5.3 software was used to analyze the data.
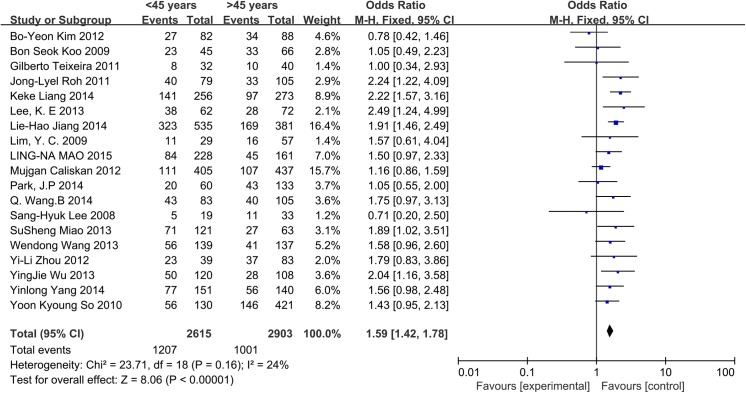
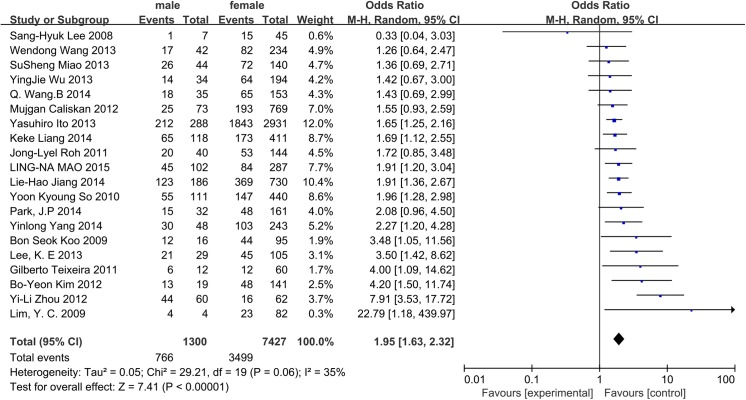
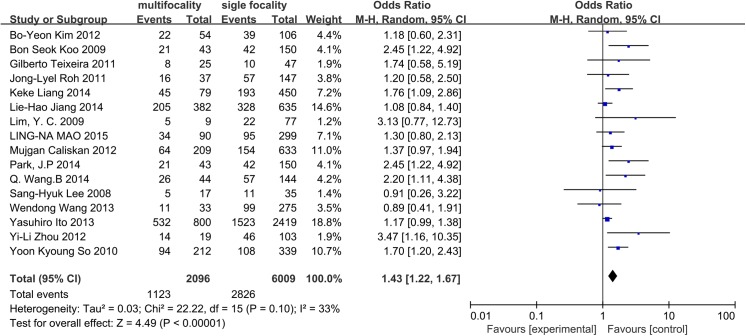
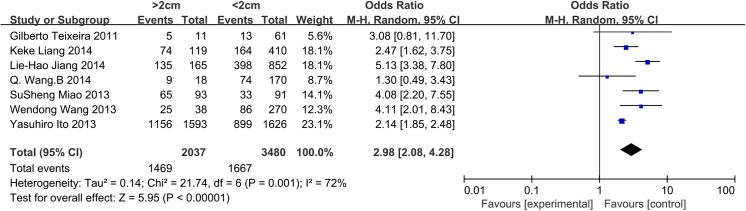
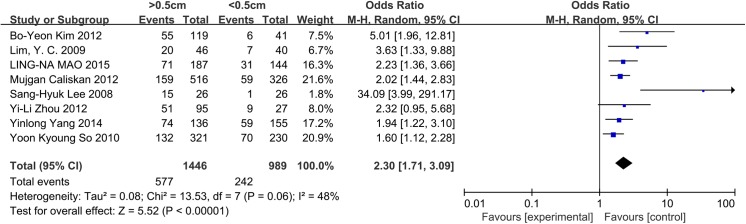
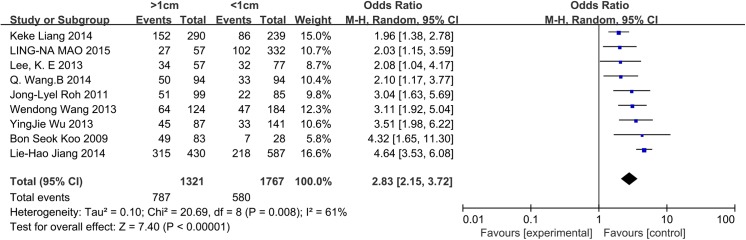
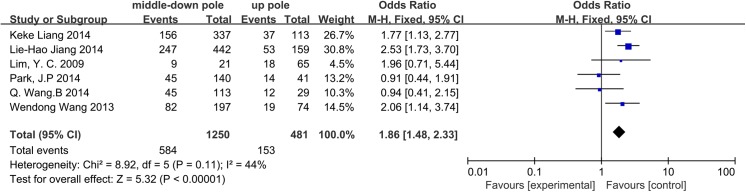
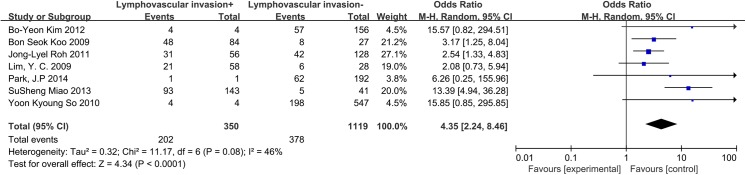
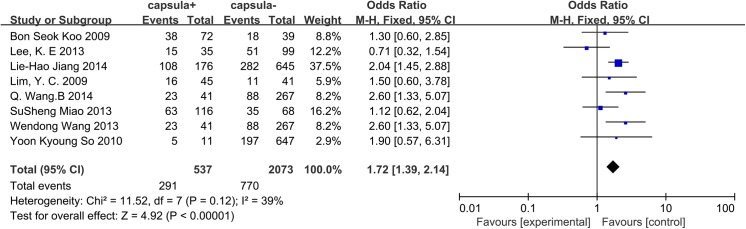
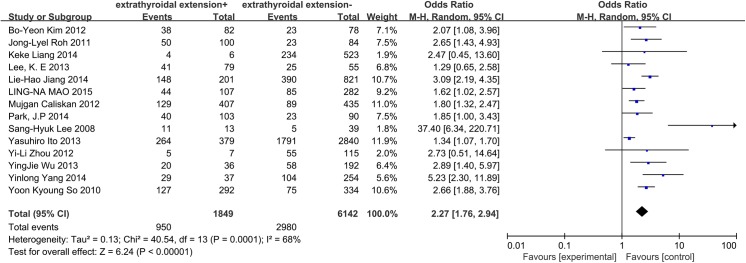
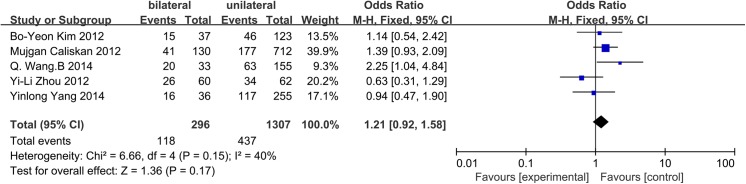
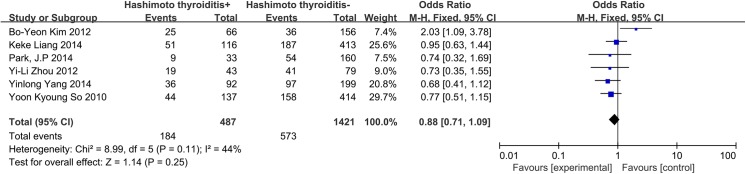
Results: Twenty studies and 9084 patients were included in this meta-analysis. The following variables were associated with an increased risk of CLNM in CN0 patients: age < 45 years (OR = 1.59, 95% CI = 1.42-1.78, p<0.00001), male sex (OR = 1.95, 95% CI = 1.63-2.32, p<0.00001), multifocality (OR = 1.43, 95% CI = 1.22-1.67, p<0.00001), tumor size > 2 cm for PTC patients (OR = 2.98, 95% CI 2.08-4.28, p<0.00001) or tumor size > 0.5 cm for papillary thyroid microcarcinoma (PTMC) patients (OR = 2.30, 95% CI = 1.71-3.09, p<0.00001), location of the primary tumor in the central area and low pole (OR = 1.86, 95% CI = 1.48-2.33, p<0.00001), lymphovascular invasion (OR = 4.35, 95% CI = 2.24-8.46, p<0.0001), extrathyroidal extension (OR = 2.27, 95% CI = 1.76-2.94, p<0.00001), and capsular invasion (OR = 1.72, 95% CI = 1.39-2.41, p<0.00001). PTC (tumor size > 1 cm) exhibited a higher risk factor associated with CLNM than PTMC (tumor size < 1 cm) (OR = 2.83, 95% CI = 2.15-3.72, p<0.00001). Bilateral tumors (OR = 1.21, 95% CI = 0.92-1.58, p = 0.17) and lymphocytic thyroiditis (OR = 0.88, 95% CI = 0.71-1.09, p = 0.25) had no association with CLNM in CN0 patients.
Conclusions: Our systematic review identified several clinical features associated with CLNM in CN0 patients, including age, sex, multifocality, size, location, lymphovascular invasion, capsular invasion, and extrathyroidal extension. These factors should guide the application of PCLND in CN0 patients.
Conflict of interest statement
Figures
Similar articles
-
The incidence and risk factors for central lymph node metastasis in cN0 papillary thyroid microcarcinoma: a meta-analysis.Eur Arch Otorhinolaryngol. 2017 Mar;274(3):1327-1338. doi: 10.1007/s00405-016-4302-0. Epub 2016 Sep 19. Eur Arch Otorhinolaryngol. 2017. PMID: 27645473 Review.
-
Identification of risk factors of central lymph node metastasis and evaluation of the effect of prophylactic central neck dissection on migration of staging and risk stratification in patients with clinically node-negative papillary thyroid microcarcinoma.Bull Cancer. 2017 Jun;104(6):516-523. doi: 10.1016/j.bulcan.2017.03.005. Epub 2017 May 2. Bull Cancer. 2017. PMID: 28476312
-
Clinical and ultrasonic risk factors for high-volume central lymph node metastasis in cN0 papillary thyroid microcarcinoma: A retrospective study and meta-analysis.Clin Endocrinol (Oxf). 2023 Apr;98(4):609-621. doi: 10.1111/cen.14834. Epub 2022 Nov 3. Clin Endocrinol (Oxf). 2023. PMID: 36263602
-
Predictive factors for central lymph node metastasis in patients with cN0 papillary thyroid carcinoma: A systematic review and meta-analysis.Int J Surg. 2016 Apr;28:153-61. doi: 10.1016/j.ijsu.2016.02.093. Epub 2016 Mar 2. Int J Surg. 2016. PMID: 26944586 Review.
-
Clinical risk factors for central lymph node metastasis in papillary thyroid carcinoma: a systematic review and meta-analysis.Clin Endocrinol (Oxf). 2015 Jul;83(1):124-32. doi: 10.1111/cen.12583. Epub 2014 Sep 22. Clin Endocrinol (Oxf). 2015. PMID: 25130203 Review.
Cited by
-
Predictive factors for non-small-volume central lymph node metastases (more than 5 or ≥ 2 mm) in clinically node-negative papillary thyroid carcinoma.Medicine (Baltimore). 2019 Jan;98(1):e14028. doi: 10.1097/MD.0000000000014028. Medicine (Baltimore). 2019. PMID: 30608456 Free PMC article.
-
Nomogram for predicting central lymph node metastasis in T1-T2 papillary thyroid cancer with no lateral lymph node metastasis.Front Endocrinol (Lausanne). 2023 Jan 19;14:1112506. doi: 10.3389/fendo.2023.1112506. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 36817601 Free PMC article.
-
Real-Time Elastography: A Web-Based Nomogram Improves the Preoperative Prediction of Central Lymph Node Metastasis in cN0 PTC.Front Oncol. 2022 Jan 13;11:755273. doi: 10.3389/fonc.2021.755273. eCollection 2021. Front Oncol. 2022. PMID: 35096569 Free PMC article.
-
Clinicopathologic Differences Between Micropapillary and Papillary Thyroid Carcinoma.Sisli Etfal Hastan Tip Bul. 2019 Apr 25;53(2):120-124. doi: 10.14744/SEMB.2019.68790. eCollection 2019. Sisli Etfal Hastan Tip Bul. 2019. PMID: 32377069 Free PMC article.
-
Nomogram Including Elastography for Prediction of Contralateral Central Lymph Node Metastasis in Solitary Papillary Thyroid Carcinoma Preoperatively.Cancer Manag Res. 2020 Oct 29;12:10789-10797. doi: 10.2147/CMAR.S278382. eCollection 2020. Cancer Manag Res. 2020. PMID: 33149684 Free PMC article.
References
-
- Lundgren CI, Hall P, Dickman PW, Zedenius J. Clinically significant prognostic factors for differentiated thyroid carcinoma: a population-based, nested case-control study. Cancer. 2006;106: 524–531. - PubMed
-
- Grebe SK, Hay ID. Thyroid cancer nodal metastases: biologic significance and therapeutic considerations. Surg Oncol Clin N Am. 1996;5: 43–63. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
