

Endocardial-epicardial distribution of myocardial perfusion reserve assessed by multidetector computed tomography in symptomatic patients without significant coronary artery disease: insights from the CORE320 multicentre study
- PMID: 26341292
- PMCID: PMC5006103
- DOI: 10.1093/ehjci/jev206
Endocardial-epicardial distribution of myocardial perfusion reserve assessed by multidetector computed tomography in symptomatic patients without significant coronary artery disease: insights from the CORE320 multicentre study
Abstract
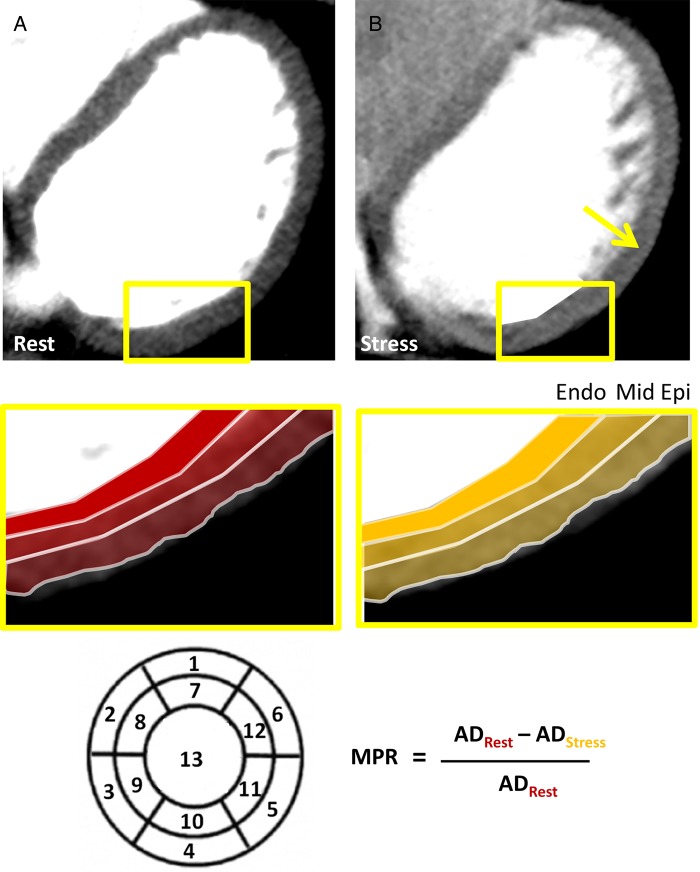
Aim: Previous animal studies have demonstrated differences in perfusion and perfusion reserve between the subendocardium and subepicardium. 320-row computed tomography (CT) with sub-millimetre spatial resolution allows for the assessment of transmural differences in myocardial perfusion reserve (MPR) in humans. We aimed to test the hypothesis that MPR in all myocardial layers is determined by age, gender, and cardiovascular risk profile in patients with ischaemic symptoms or equivalent but without obstructive coronary artery disease (CAD).
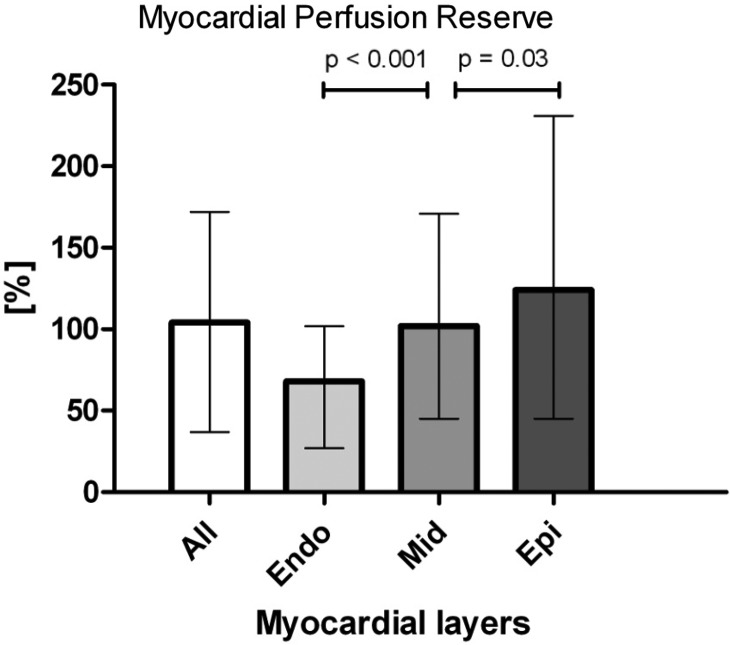
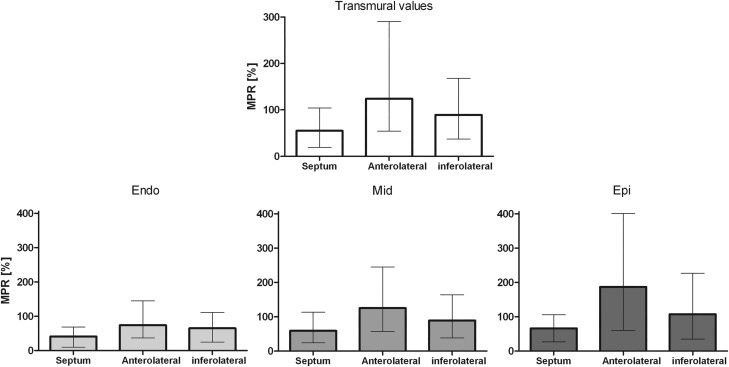
Methods and results: A total of 149 patients enrolled in the CORE320 study with symptoms or signs of myocardial ischaemia and absence of significant CAD by invasive coronary angiography were scanned with static rest and stress CT perfusion. Myocardial attenuation densities were assessed at rest and during adenosine stress, segmented into 3 myocardial layers and 13 segments. MPR was higher in the subepicardium compared with the subendocardium (124% interquartile range [45, 235] vs. 68% [22,102], P < 0.001). Moreover, MPR in the septum was lower than in the inferolateral and anterolateral segments of the myocardium (55% [19, 104] vs. 89% [37, 168] and 124% [54, 270], P < 0.001). By multivariate analysis, high body mass index was significantly associated with reduced MPR in all myocardial layers when adjusted for cardiovascular risk factors (P = 0.02).
Conclusion: In symptomatic patients without significant coronary artery stenosis, distinct differences in endocardial-epicardial distribution of perfusion reserve may be demonstrated with static CT perfusion. Low MPR in all myocardial layers was observed specifically in obese patients.
Keywords: coronary artery disease; multi-detector computed tomography; myocardial perfusion.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2015. For permissions please email: journals.permissions@oup.com.
Figures

Similar articles
-
Lack of association between epicardial fat volume and extent of coronary artery calcification, severity of coronary artery disease, or presence of myocardial perfusion abnormalities in a diverse, symptomatic patient population: results from the CORE320 multicenter study.Circ Cardiovasc Imaging. 2015 Mar;8(3):e002676. doi: 10.1161/CIRCIMAGING.114.002676. Circ Cardiovasc Imaging. 2015. PMID: 25752899 Free PMC article.
-
SPECT Myocardial Perfusion Reserve in Patients with Multivessel Coronary Disease: Correlation with Angiographic Findings and Invasive Fractional Flow Reserve Measurements.J Nucl Med. 2015 Nov;56(11):1712-7. doi: 10.2967/jnumed.114.143164. Epub 2015 Sep 3. J Nucl Med. 2015. PMID: 26338893
-
Diagnostic value of global myocardial perfusion reserve assessment based on coronary sinus flow measurements using cardiovascular magnetic resonance in addition to myocardial stress perfusion imaging.Eur Heart J Cardiovasc Imaging. 2017 May 1;18(8):851-859. doi: 10.1093/ehjci/jew315. Eur Heart J Cardiovasc Imaging. 2017. PMID: 28369259
-
Meta-Analysis of Diagnostic Performance of Coronary Computed Tomography Angiography, Computed Tomography Perfusion, and Computed Tomography-Fractional Flow Reserve in Functional Myocardial Ischemia Assessment Versus Invasive Fractional Flow Reserve.Am J Cardiol. 2015 Nov 1;116(9):1469-78. doi: 10.1016/j.amjcard.2015.07.078. Epub 2015 Aug 14. Am J Cardiol. 2015. PMID: 26347004 Free PMC article. Review.
-
CT-based myocardial ischemia evaluation: quantitative angiography, transluminal attenuation gradient, myocardial perfusion, and CT-derived fractional flow reserve.Int J Cardiovasc Imaging. 2016 Jun;32 Suppl 1:1-19. doi: 10.1007/s10554-015-0825-5. Epub 2015 Dec 14. Int J Cardiovasc Imaging. 2016. PMID: 26667445 Review.
Cited by
-
Quantitative Assessment of Coronary Microvascular Function: Dynamic Single-Photon Emission Computed Tomography, Positron Emission Tomography, Ultrasound, Computed Tomography, and Magnetic Resonance Imaging.Circ Cardiovasc Imaging. 2017 Aug;10(8):e006427. doi: 10.1161/CIRCIMAGING.117.006427. Circ Cardiovasc Imaging. 2017. PMID: 28794138 Free PMC article. Review.
-
Coronary Microvascular Dysfunction: PET, CMR and CT Assessment.J Clin Med. 2021 Apr 23;10(9):1848. doi: 10.3390/jcm10091848. J Clin Med. 2021. PMID: 33922841 Free PMC article. Review.
-
Diagnostic value of quantitative parameters for myocardial perfusion assessment in patients with suspected coronary artery disease by single- and dual-energy computed tomography myocardial perfusion imaging.Int J Cardiol Heart Vasc. 2021 Feb 4;32:100721. doi: 10.1016/j.ijcha.2021.100721. eCollection 2021 Feb. Int J Cardiol Heart Vasc. 2021. PMID: 33604450 Free PMC article.
-
Clinical quantitative cardiac imaging for the assessment of myocardial ischaemia.Nat Rev Cardiol. 2020 Jul;17(7):427-450. doi: 10.1038/s41569-020-0341-8. Epub 2020 Feb 24. Nat Rev Cardiol. 2020. PMID: 32094693 Free PMC article.
-
Evaluation of computed tomography myocardial perfusion in women with angina and no obstructive coronary artery disease.Int J Cardiovasc Imaging. 2020 Feb;36(2):367-382. doi: 10.1007/s10554-019-01723-5. Epub 2019 Nov 1. Int J Cardiovasc Imaging. 2020. PMID: 31676944
References
-
- Reimer KA, Lowe JE, Rasmussen MM, Jennings RB. The wavefront phenomenon of ischemic cell death. 1. Myocardial infarct size vs. duration of coronary occlusion in dogs. Circulation 1977;56:786–94. - PubMed
-
- Duncker DJ, Bache RJ. Regulation of coronary blood flow during exercise. Physiol Rev 2008;88:1009–86. - PubMed
-
- Schindler TH, Schelbert HR, Quercioli A, Dilsizian V. Cardiac PET imaging for the detection and monitoring of coronary artery disease and microvascular health. JACC Cardiovasc Imaging 2010;3:623–40. - PubMed
-
- Schindler TH, Nitzsche EU, Schelbert HR, Olschewski M, Sayre J, Mix M et al. . Positron emission tomography-measured abnormal responses of myocardial blood flow to sympathetic stimulation are associated with the risk of developing cardiovascular events. J Am Coll Cardiol 2005;45:1505–12. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
