

Misclassification of acute respiratory distress syndrome after traumatic injury: The cost of less rigorous approaches
- PMID: 26307875
- PMCID: PMC4552075
- DOI: 10.1097/TA.0000000000000760
Misclassification of acute respiratory distress syndrome after traumatic injury: The cost of less rigorous approaches
Abstract
Background: Adherence to rigorous research protocols for identifying adult respiratory distress syndrome (ARDS) after trauma is variable. To examine how misclassification of ARDS may bias observational studies in trauma populations, we evaluated the agreement of two methods for adjudicating ARDS after trauma: the current gold standard, direct review of chest radiographs and review of dictated radiology reports, a commonly used alternative.
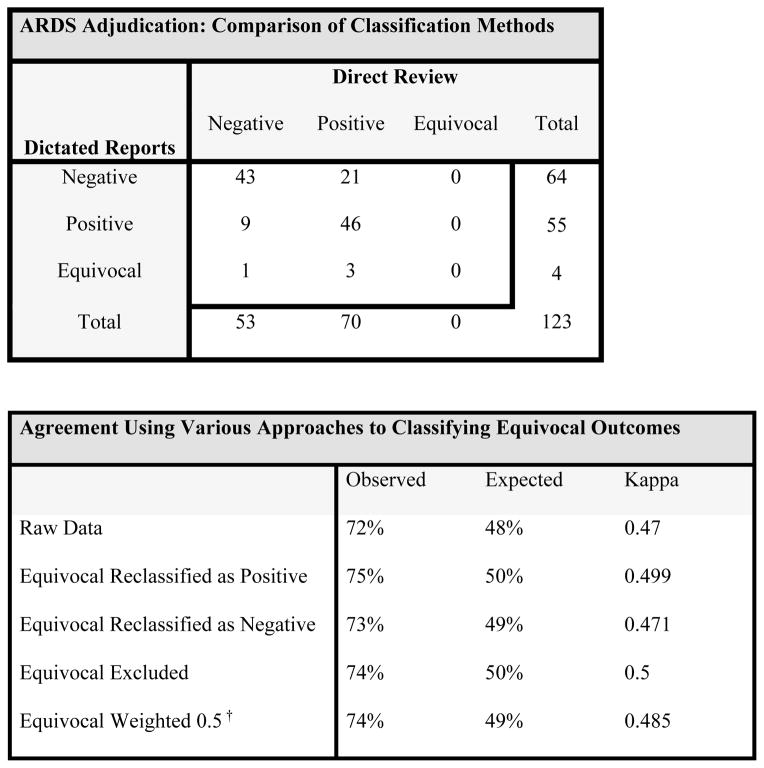
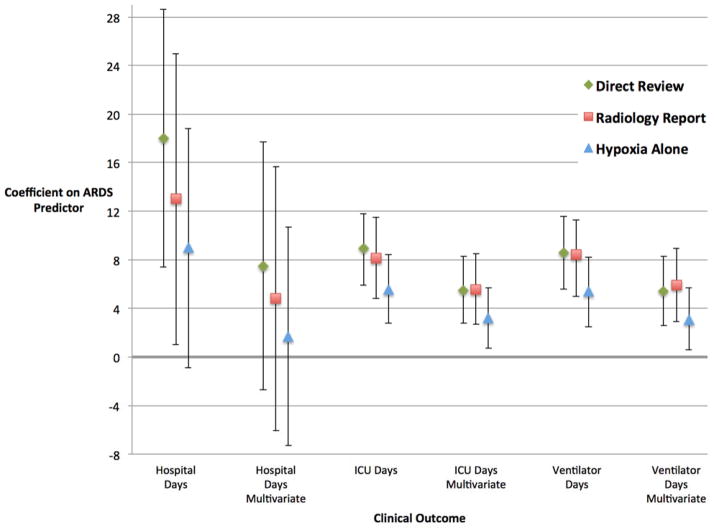
Methods: This nested cohort study included 123 mechanically ventilated patients between 2005 and 2008, with at least one PaO2/FIO2 less than 300 within the first 8 days of admission. Two blinded physician investigators adjudicated ARDS by two methods. The investigators directly reviewed all chest radiographs to evaluate for bilateral infiltrates. Several months later, blinded to their previous assessments, they adjudicated ARDS using a standardized rubric to classify radiology reports. A κ statistics was calculated. Regression analyses quantified the association between established risk factors as well as important clinical outcomes and ARDS determined by the aforementioned methods as well as hypoxemia as a surrogate marker.
Results: The κ was 0.47 for the observed agreement between ARDS adjudicated by direct review of chest radiographs and ARDS adjudicated by review of radiology reports. Both the magnitude and direction of bias on the estimates of association between ARDS and established risk factors as well as clinical outcomes varied by method of adjudication.
Conclusion: Classification of ARDS by review of dictated radiology reports had only moderate agreement with the current gold standard, ARDS adjudicated by direct review of chest radiographs. While the misclassification of ARDS had varied effects on the estimates of associations with established risk factors, it tended to weaken the association of ARDS with important clinical outcomes. A standardized approach to ARDS adjudication after trauma by direct review of chest radiographs will minimize misclassification bias in future observational studies.
Level of evidence: Diagnostic study, level II.
Conflict of interest statement
Conflicts of Interest: The authors have no relevant conflicts of interest to disclose.
Figures
Similar articles
-
Differences in degree, differences in kind: characterizing lung injury in trauma.J Trauma Acute Care Surg. 2015 Apr;78(4):735-41. doi: 10.1097/TA.0000000000000583. J Trauma Acute Care Surg. 2015. PMID: 25742257 Free PMC article.
-
Thoracic Trauma Severity score on admission allows to determine the risk of delayed ARDS in trauma patients with pulmonary contusion.Injury. 2016 Jan;47(1):147-53. doi: 10.1016/j.injury.2015.08.031. Epub 2015 Aug 29. Injury. 2016. PMID: 26358517
-
Modelling thirty-day mortality in the Acute Respiratory Distress Syndrome (ARDS) in an adult ICU.Anaesth Intensive Care. 2004 Jun;32(3):317-29. doi: 10.1177/0310057X0403200304. Anaesth Intensive Care. 2004. PMID: 15264725
-
Acute Respiratory Distress Syndrome: Advances in Diagnosis and Treatment.JAMA. 2018 Feb 20;319(7):698-710. doi: 10.1001/jama.2017.21907. JAMA. 2018. PMID: 29466596 Review.
-
[Ventilatory strategy for ARDS].Nihon Rinsho. 2016 Feb;74(2):279-84. Nihon Rinsho. 2016. PMID: 26915253 Review. Japanese.
Cited by
-
Acute Respiratory Distress Syndrome Measurement Error. Potential Effect on Clinical Study Results.Ann Am Thorac Soc. 2016 Jul;13(7):1123-8. doi: 10.1513/AnnalsATS.201601-072OC. Ann Am Thorac Soc. 2016. PMID: 27159648 Free PMC article.
-
Health care utilization and the cost of posttraumatic acute respiratory distress syndrome care.J Trauma Acute Care Surg. 2018 Jul;85(1):148-154. doi: 10.1097/TA.0000000000001926. J Trauma Acute Care Surg. 2018. PMID: 29958249 Free PMC article.
-
Possible Predictive Factor of Acute Respiratory Distress Syndrome Development After Mild Traumatic Brain Injury: A Single Rural Trauma Center Preliminary Study.Cureus. 2021 Jul 20;13(7):e16508. doi: 10.7759/cureus.16508. eCollection 2021 Jul. Cureus. 2021. PMID: 34430122 Free PMC article.
-
Cigarette Smoking and ARDS After Blunt Trauma: The Influence of Changing Smoking Patterns and Resuscitation Practices.Chest. 2020 Oct;158(4):1490-1498. doi: 10.1016/j.chest.2020.05.603. Epub 2020 Jun 20. Chest. 2020. PMID: 32574574 Free PMC article.
-
The acute respiratory distress syndrome following isolated severe traumatic brain injury.J Trauma Acute Care Surg. 2016 Jun;80(6):989-97. doi: 10.1097/TA.0000000000000982. J Trauma Acute Care Surg. 2016. PMID: 26881489 Free PMC article.
References
-
- Rubenfeld GD, Caldwell E, Peabody E, Weaver J, Martin DP, Neff M, Stern EJ, Hudson LD. Incidence and outcomes of acute lung injury. N Engl J Med. 2005;353(16):1685–1693. - PubMed
-
- Shah CVLA, Lanken PN, Kahn JM, Bellamy S, Gallop R, Finkel B, Gracias VH, Fuchs BD, Christie JD. The impact of development of acute lung injury on hospital mortality in critically ill trauma patients. Crit Care Med. 2008;36:2309–2315. - PubMed
-
- Guerin C, Reignier J, Richard JC. Prone positioning in the acute respiratory distress syndrome. New Engl J Med. 2013;369(10):980–981. - PubMed
-
- National Heart L, Blood Institute Acute Respiratory Distress Syndrome Clinical Trials N. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. New Engl J Med. 2000;342(18):1301–1308. - PubMed
-
- National Heart L, Blood Institute Acute Respiratory Distress Syndrome Clinical Trials N. Wiedemann HP, et al. Comparison of two fluid-management strategies in acute lung injury. The New Engl J Med. 2006;354(24):2564–2575. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
