

A Diabetic Emergency One Million Feet Long: Disparities and Burdens of Illness among Diabetic Foot Ulcer Cases within Emergency Departments in the United States, 2006-2010
- PMID: 26248037
- PMCID: PMC4527828
- DOI: 10.1371/journal.pone.0134914
A Diabetic Emergency One Million Feet Long: Disparities and Burdens of Illness among Diabetic Foot Ulcer Cases within Emergency Departments in the United States, 2006-2010
Abstract
Objectives: To evaluate the magnitude and impact of diabetic foot ulcers (DFUs) in emergency department (ED) settings from 2006-2010 in the United States (US).
Methods: This cross-sectional study utilized Agency for Healthcare Research and Quality (AHRQ) Healthcare Cost and Utilization Project (HCUP) National Emergency Department Sample (NEDS) discharge records of ED cases among persons ≥18 years with any-listed diagnosis of DFUs. Multivariable analyses were conducted for clinical outcomes of patient disposition from the ED and economic outcomes of charges and lengths of stay based upon patient demographic and socioeconomic factors, hospital characteristics, and comorbid disease states.
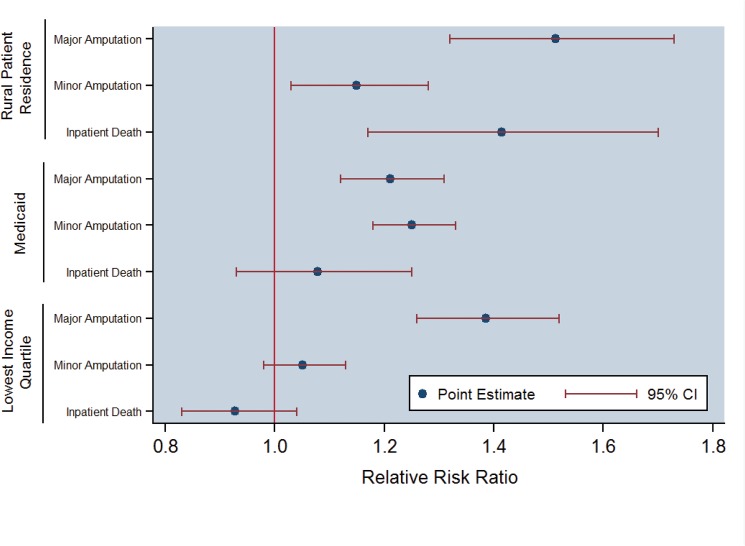
Results: Overall, 1,019,861 cases of diabetic foot complications presented to EDs in the US from 2006-2010, comprising 1.9% of the 54.2 million total diabetes cases. The mean patient age was 62.5 years and 59.4% were men. The national bill was $1.9 billion per year in the ED and $8.78 billion per year (US$ 2014) including inpatient charges among the 81.2% of cases that were admitted. Clinical outcomes included mortality in 2.0%, sepsis in 9.6% of cases and amputation in 10.5% (major-minor amputation ratio of 0.46). Multivariable analyses found that those residing in non-urban locations were associated with +51.3%, +14.9%, and +41.4% higher odds of major amputation, minor amputation, and inpatient death, respectively (p<0.05). Medicaid beneficiaries incurred +21.1% and +25.1% higher odds for major or minor amputations, respectively, than Medicare patients (p<0.05). Persons within the lowest income quartile regions were associated with a +38.5% higher odds of major amputation (p<0.05) versus the highest income regions.
Conclusion: Diabetic foot complications exact a substantial clinical and economic toll in acute care settings, particularly among the rural and working poor. Clear opportunities exist to reduce costs and improve outcomes for this systematically-neglected condition by establishing effective practice paradigms for screening, prevention, and coordinated care.
Conflict of interest statement
Figures
Similar articles
-
Trends and determinants of costs associated with the inpatient care of diabetic foot ulcers.J Vasc Surg. 2014 Nov;60(5):1247-1254.e2. doi: 10.1016/j.jvs.2014.05.009. Epub 2014 Jun 14. J Vasc Surg. 2014. PMID: 24939079 Free PMC article.
-
Open bypass and endovascular procedures among diabetic foot ulcer cases in the United States from 2001 to 2010.J Vasc Surg. 2014 Nov;60(5):1255-1265. doi: 10.1016/j.jvs.2014.04.071. Epub 2014 Jul 11. J Vasc Surg. 2014. PMID: 25017514
-
The costs of diabetic foot: the economic case for the limb salvage team.J Vasc Surg. 2010 Sep;52(3 Suppl):17S-22S. doi: 10.1016/j.jvs.2010.06.003. J Vasc Surg. 2010. PMID: 20804928 Review.
-
Analyzing treatment aggressiveness and identifying high-risk patients in diabetic foot ulcer return to care.Wound Repair Regen. 2016 Jul;24(4):731-6. doi: 10.1111/wrr.12439. Epub 2016 Jun 8. Wound Repair Regen. 2016. PMID: 27144893
-
Losing a foot versus losing a dollar; a systematic review of cost studies in diabetic foot complications.Expert Rev Pharmacoecon Outcomes Res. 2017 Apr;17(2):165-180. doi: 10.1080/14737167.2017.1305891. Epub 2017 Mar 17. Expert Rev Pharmacoecon Outcomes Res. 2017. PMID: 28283002 Review.
Cited by
-
Investigating auranofin for the treatment of infected diabetic pressure ulcers in mice and dermal toxicity in pigs.Sci Rep. 2021 May 25;11(1):10935. doi: 10.1038/s41598-021-90360-x. Sci Rep. 2021. PMID: 34035383 Free PMC article.
-
The current burden of diabetic foot disease.J Clin Orthop Trauma. 2021 Feb 8;17:88-93. doi: 10.1016/j.jcot.2021.01.017. eCollection 2021 Jun. J Clin Orthop Trauma. 2021. PMID: 33680841 Free PMC article.
-
Smart Offloading Boot System for Remote Patient Monitoring: Toward Adherence Reinforcement and Proper Physical Activity Prescription for Diabetic Foot Ulcer Patients.J Diabetes Sci Technol. 2023 Jan;17(1):42-51. doi: 10.1177/19322968211070850. Epub 2022 Jan 20. J Diabetes Sci Technol. 2023. PMID: 35048739 Free PMC article.
-
Increasing SBP variability is associated with an increased risk of developing incident diabetic foot ulcers.J Hypertens. 2018 Nov;36(11):2177-2184. doi: 10.1097/HJH.0000000000001783. J Hypertens. 2018. PMID: 29794815 Free PMC article.
-
Early intervention and care for Diabetic Foot Ulcers in Low and Middle Income Countries: Addressing challenges and exploring future strategies: A narrative review.Health Sci Rep. 2024 Apr 29;7(5):e2075. doi: 10.1002/hsr2.2075. eCollection 2024 May. Health Sci Rep. 2024. PMID: 38690005 Free PMC article.
References
-
- Boulton AJM, Vileikyte L, Ragnarson-Tennvall G, Apelqvist J. The global burden of diabetic foot disease. Lancet 2005;366:1719–24. - PubMed
-
- Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA 2005;293:217–28. - PubMed
-
- Lavery LA, Armstrong DG, Wunderlich RP, Mohler MJ, Wendel CS, Lipsky BA. Risk factors for foot infections in individuals with diabetes. Diabetes Care 2006;29:1288–93. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
