

Review
doi: 10.1126/scitranslmed.aaa7322.
Immune-mediated pathology in Duchenne muscular dystrophy
Affiliations
- PMID: 26246170
- PMCID: PMC5951380
- DOI: 10.1126/scitranslmed.aaa7322
Item in Clipboard
Review
Immune-mediated pathology in Duchenne muscular dystrophy
Sci Transl Med.
.
Abstract
Immunological and inflammatory processes downstream of dystrophin deficiency as well as metabolic abnormalities, defective autophagy, and loss of regenerative capacity all contribute to muscle pathology in Duchenne muscular dystrophy (DMD). These downstream cascades offer potential avenues for pharmacological intervention. Modulating the inflammatory response and inducing immunological tolerance to de novo dystrophin expression will be critical to the success of dystrophin-replacement therapies. This Review focuses on the role of the inflammatory response in DMD pathogenesis and opportunities for clinical intervention.
Copyright © 2015, American Association for the Advancement of Science.
Figures
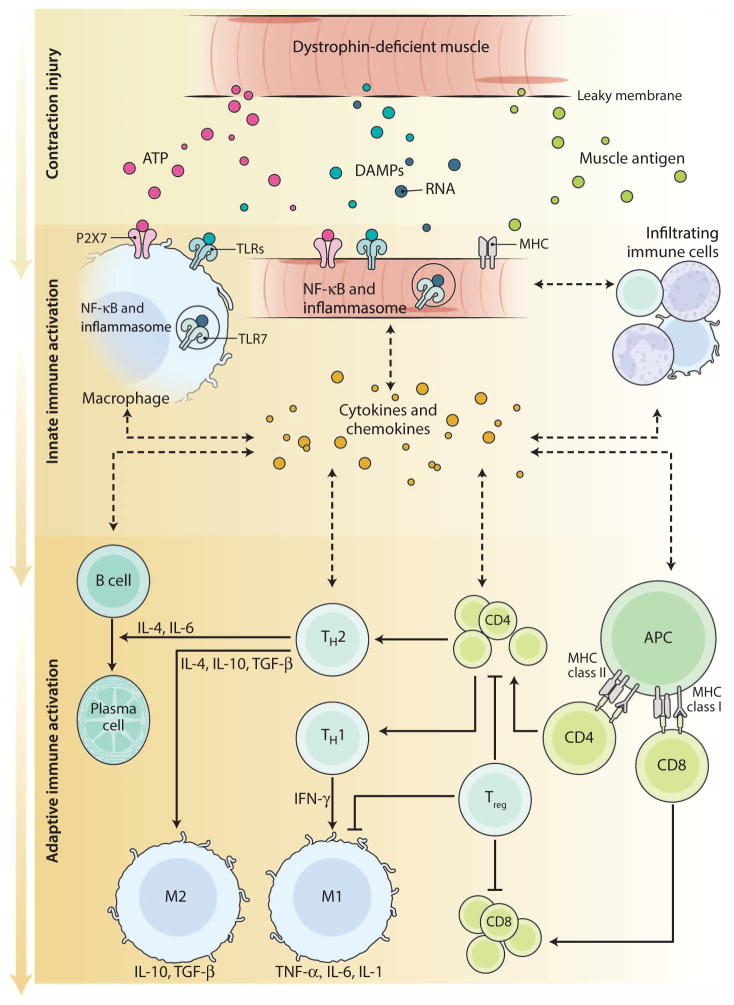
Dystrophin-deficient muscle cells are susceptible to contraction-induced injury, culminating in muscle necrosis and the release of DAMP molecules including ATP (adenosine 5′-triphosphate) and nucleic acids. Released muscle proteins may serve as neoantigens. Engagement by DAMPs of TLR7 and the ionotropic receptor P2X7 on skeletal muscle cells and macrophages triggers innate immune activation and a chronic inflammatory response. Concomitantly, MHC presentation of peptides derived from muscle antigens initiates an adaptive immune response. Cytokines and chemokines released in the milieu attract and activate additional infiltrating immune cells including neutrophils and antigen presenting cells (APCs), such as M1 macrophages and dendritic cells. The APCs, in turn, activate recruited lymphocytes (CD4+ and CD8+ T cells), leading to propagation of adaptive immune responses (TH1, TH2), which are dampened by Tregs. Although B cells have been detected in DMD muscle, there is no known role for B cells in antigen presentation or antibody production in the context of DMD. The balance between the TH1 and the TH2 adaptive immune response creates a regulatory feedback mechanism that leads to activation of either M1 or M2 macrophages, which affects the severity of muscle inflammation or the efficiency of muscle regeneration, respectively.
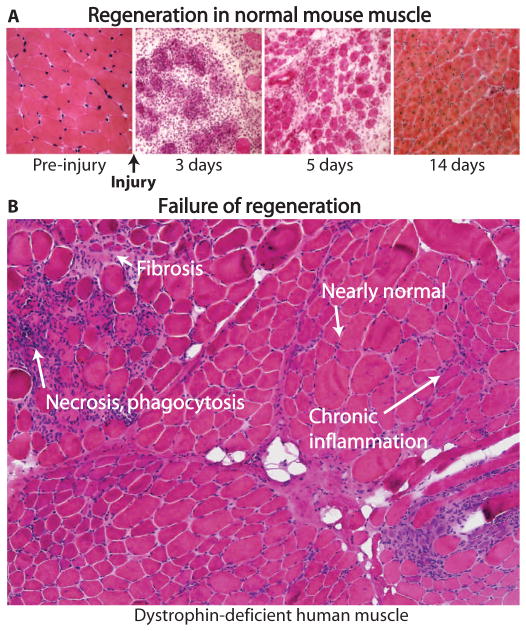
(A) Stages of regeneration in normal mouse muscle after injury. Regeneration of skeletal muscle in response to injury is a highly synchronized process. Within 24 hours of injury, mouse muscle becomes infiltrated with neutrophils. Within 2 to 3 days, the injured muscle is infiltrated by pro-inflammatory M1 macrophages. During days 5 to 10, the resolution and repair phases of regeneration take place and muscle is predominantly populated by remodeling M2 macrophages. M2 macrophages are essential for complete muscle regeneration, which is achieved by day 14. (B) Asynchronous degeneration/regeneration in human dystrophin-deficient muscle. Repair of human dystrophin-deficient muscle after injury is impaired due to asynchronous bouts of degeneration and regeneration, leading to the release of cytokines, such as TGF-β, that initiate and perpetuate fibrosis. Shown is a muscle biopsy from a DMD patient revealing regions of nearly normal myofibers; chronic inflammation (between myofibers); phagocytosis by neutrophils and macrophages, and necrosis; and fibrosis (failed regeneration).
Similar articles
-
Skeletal Muscle Differentiation on a Chip Shows Human Donor Mesoangioblasts' Efficiency in Restoring Dystrophin in a Duchenne Muscular Dystrophy Model.Stem Cells Transl Med. 2016 Dec;5(12):1676-1683. doi: 10.5966/sctm.2015-0053. Epub 2016 Aug 8. Stem Cells Transl Med. 2016. PMID: 27502519 Free PMC article.
-
Pharmacological prospects in the treatment of Duchenne muscular dystrophy.Curr Opin Neurol. 2013 Oct;26(5):577-84. doi: 10.1097/WCO.0b013e328364fbaf. Curr Opin Neurol. 2013. PMID: 23995279 Review.
-
Drug Discovery of Therapies for Duchenne Muscular Dystrophy.J Biomol Screen. 2015 Dec;20(10):1189-203. doi: 10.1177/1087057115586535. Epub 2015 May 14. J Biomol Screen. 2015. PMID: 25975656 Review.
-
Alterations in Notch signalling in skeletal muscles from mdx and dko dystrophic mice and patients with Duchenne muscular dystrophy.Exp Physiol. 2014 Apr;99(4):675-87. doi: 10.1113/expphysiol.2013.077255. Epub 2014 Jan 17. Exp Physiol. 2014. PMID: 24443351
-
The role of branched fibres in the pathogenesis of Duchenne muscular dystrophy.Exp Physiol. 2011 Jun;96(6):564-71. doi: 10.1113/expphysiol.2010.056713. Epub 2011 Mar 18. Exp Physiol. 2011. PMID: 21421700 Review.
Cited by
-
High mobility group box 1 (HMGB1) is a potential disease biomarker in cell and mouse models of Duchenne muscular dystrophy.Biol Open. 2024 Sep 15;13(9):bio060542. doi: 10.1242/bio.060542. Epub 2024 Sep 5. Biol Open. 2024. PMID: 39158383 Free PMC article.
-
Report of a TREAT-NMD/World Duchenne Organisation Meeting on Dystrophin Quantification Methodology.J Neuromuscul Dis. 2019;6(1):147-159. doi: 10.3233/JND-180357. J Neuromuscul Dis. 2019. PMID: 30614809 Free PMC article.
-
CD38-NADase is a new major contributor to Duchenne muscular dystrophic phenotype.EMBO Mol Med. 2022 May 9;14(5):e12860. doi: 10.15252/emmm.202012860. Epub 2022 Mar 17. EMBO Mol Med. 2022. PMID: 35298089 Free PMC article.
-
Phase IIa trial in Duchenne muscular dystrophy shows vamorolone is a first-in-class dissociative steroidal anti-inflammatory drug.Pharmacol Res. 2018 Oct;136:140-150. doi: 10.1016/j.phrs.2018.09.007. Epub 2018 Sep 13. Pharmacol Res. 2018. PMID: 30219580 Free PMC article. Clinical Trial.
-
Mouse models of NADK2 deficiency analyzed for metabolic and gene expression changes to elucidate pathophysiology.Hum Mol Genet. 2022 Nov 28;31(23):4055-4074. doi: 10.1093/hmg/ddac151. Hum Mol Genet. 2022. PMID: 35796562 Free PMC article.
References
-
- National Center for Immunization, Respiratory Diseases. General recommendations on immunization—Recommendations of the Advisory Committee on Immunization Practices (ACIP) MMWR Recomm Rep. 2011;60:1–64. - PubMed
-
- Pétrilli V, Dostert C, Muruve DA, Tschopp J. The inflammasome: A danger sensing complex triggering innate immunity. Curr Opin Immunol. 2007;19:615–622. - PubMed
-
- Hyldahl RD, Nelson B, Xin L, Welling T, Groscost L, Hubal MJ, Chipkin S, Clarkson PM, Parcell AC. Extracellular matrix remodeling and its contribution to protective adaptation following lengthening contractions in human muscle. FASEB J. 2015;29:2894–2904. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
