

Progress in Small Molecule Therapeutics for the Treatment of Retinoblastoma
- PMID: 26202204
- PMCID: PMC5509337
- DOI: 10.2174/1389557515666150722100610
Progress in Small Molecule Therapeutics for the Treatment of Retinoblastoma
Abstract
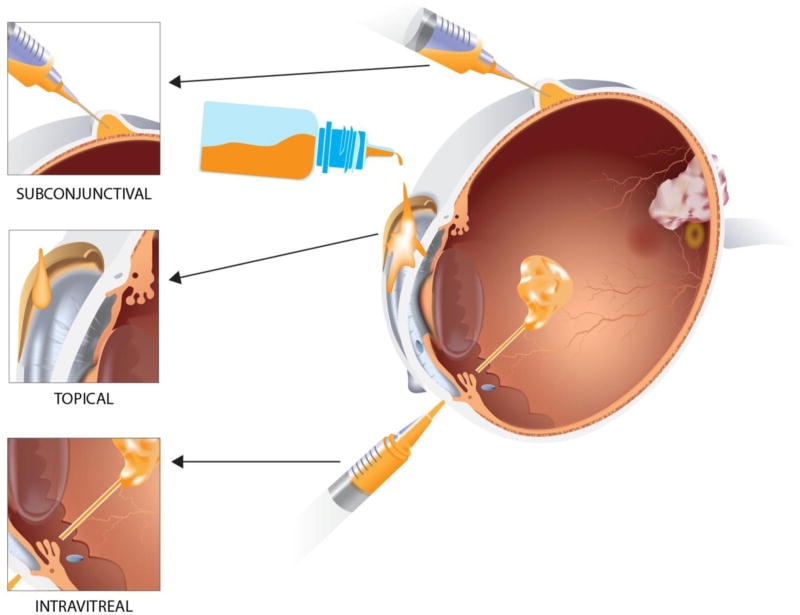
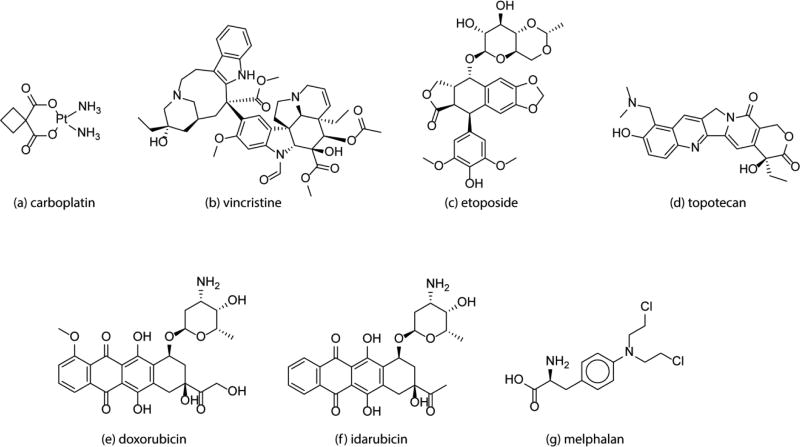
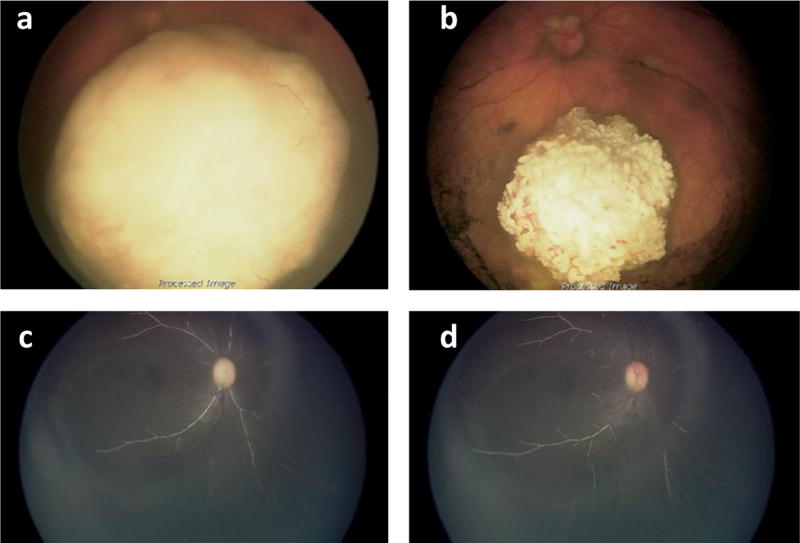
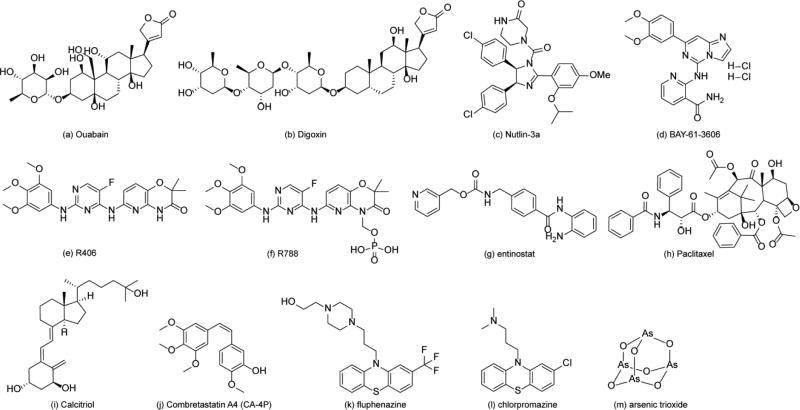
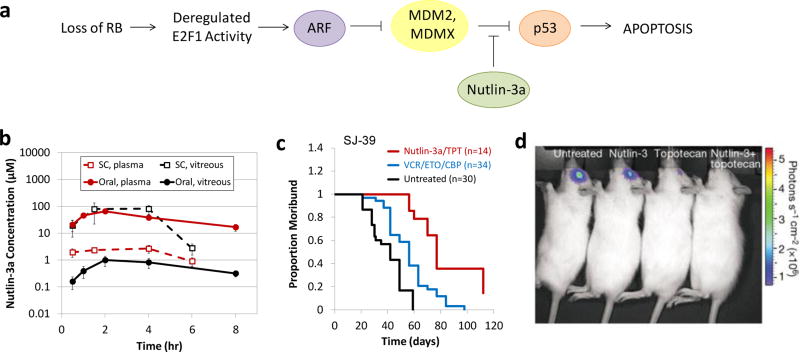
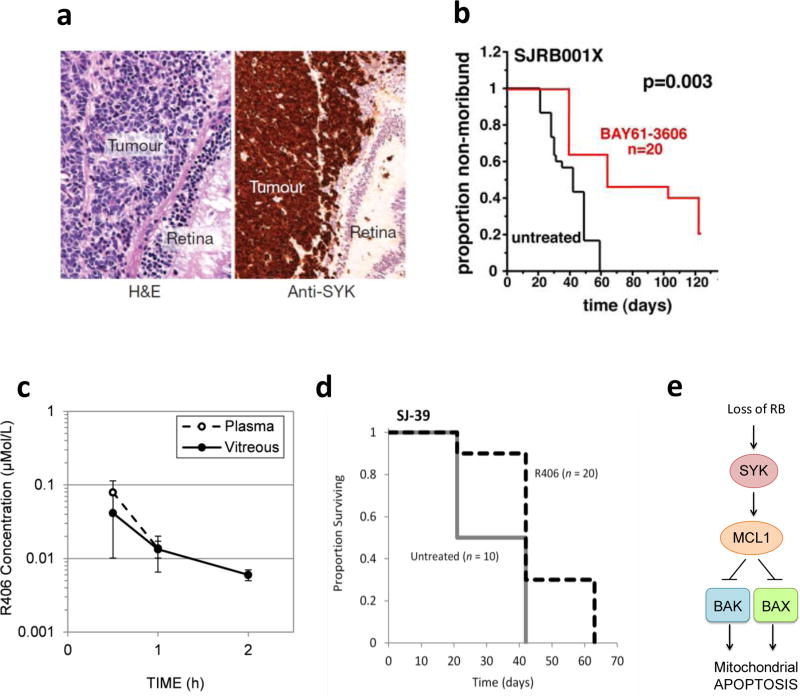
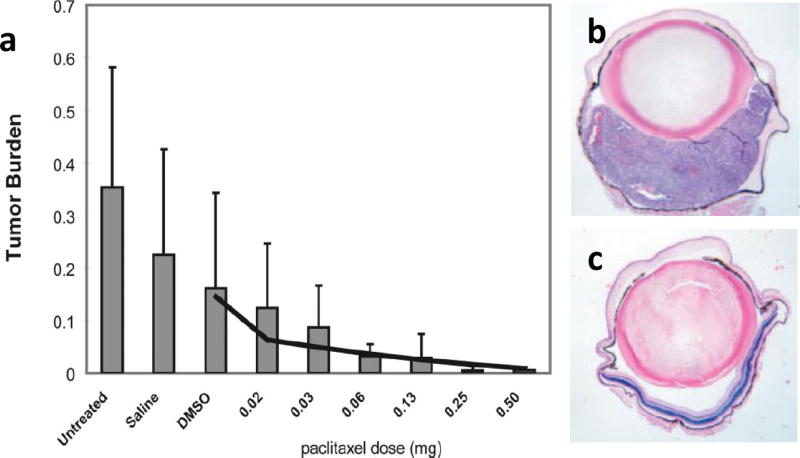
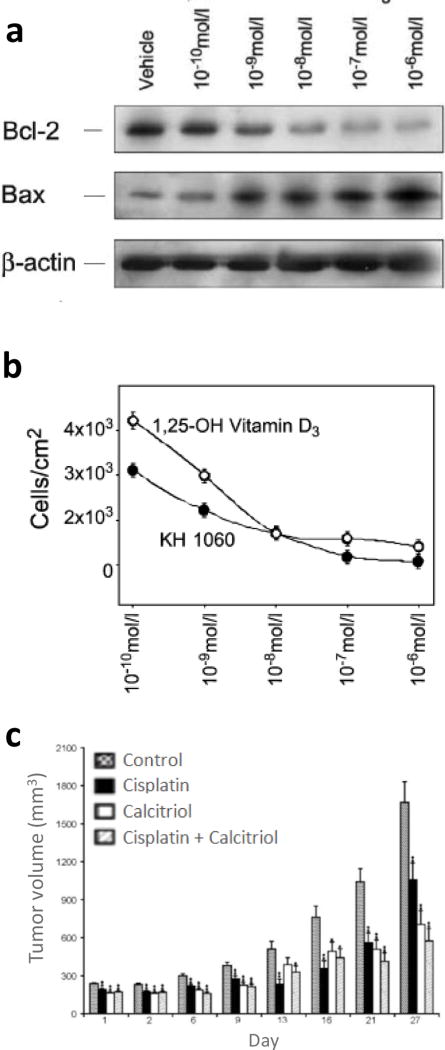
While mortality is low for intraocular retinoblastoma patients in the developed world who receive aggressive multimodal therapy, partial or full loss of vision occurs in approximately 50% of patients with advanced bilateral retinoblastoma. Therapies that preserve vision and reduce late effects are needed. Because clinical trials for retinoblastoma are difficult due to the young age of the patient population and relative rarity of the disease, robust preclinical testing of new therapies is critical. The last decade has seen advances towards identifying new therapies including the development of animal models of retinoblastoma for preclinical testing, progress in local drug delivery to reach intraocular targets, and improved understanding of the underlying biological mechanisms that give rise to retinoblastoma. This review discusses advances in these areas, with a focus on discovery and development of small molecules for the treatment of retinoblastoma, including novel targeted therapeutics such as inhibitors of the MDMX-p53 interaction (nutlin-3a), histone deacetylase (HDAC) inhibitors, and spleen tyrosine kinase (SYK) inhibitors.
Conflict of interest statement
Figures
Similar articles
-
Pharmacokinetics and efficacy of the spleen tyrosine kinase inhibitor r406 after ocular delivery for retinoblastoma.Pharm Res. 2014 Nov;31(11):3060-72. doi: 10.1007/s11095-014-1399-y. Epub 2014 Jun 7. Pharm Res. 2014. PMID: 24906597 Free PMC article.
-
Targeting the p53 pathway in retinoblastoma with subconjunctival Nutlin-3a.Cancer Res. 2011 Jun 15;71(12):4205-13. doi: 10.1158/0008-5472.CAN-11-0058. Epub 2011 Apr 22. Cancer Res. 2011. PMID: 21515735 Free PMC article.
-
Small molecule inhibition of HDM2 leads to p53-mediated cell death in retinoblastoma cells.Arch Ophthalmol. 2006 Sep;124(9):1269-75. doi: 10.1001/archopht.124.9.1269. Arch Ophthalmol. 2006. PMID: 16966622
-
Targeting MDM2 and MDMX in retinoblastoma.Curr Cancer Drug Targets. 2007 Nov;7(7):689-95. doi: 10.2174/156800907782418266. Curr Cancer Drug Targets. 2007. PMID: 18045074 Review.
-
Small-molecule MDM2-p53 inhibitors: recent advances.Future Med Chem. 2015;7(5):631-45. doi: 10.4155/fmc.15.13. Future Med Chem. 2015. PMID: 25921402 Review.
Cited by
-
Characterization and Molecular Mechanism of Peptide-Conjugated Gold Nanoparticle Inhibiting p53-HDM2 Interaction in Retinoblastoma.Mol Ther Nucleic Acids. 2017 Dec 15;9:349-364. doi: 10.1016/j.omtn.2017.10.012. Epub 2017 Oct 20. Mol Ther Nucleic Acids. 2017. PMID: 29246314 Free PMC article.
-
VEGF overexpression is associated with optic nerve involvement and differentiation of retinoblastoma: A PRISMA-compliant meta-analysis.Medicine (Baltimore). 2018 Dec;97(51):e13753. doi: 10.1097/MD.0000000000013753. Medicine (Baltimore). 2018. PMID: 30572521 Free PMC article.
-
microRNA -378a-3p Restrains the Proliferation of Retinoblastoma Cells but Promotes Apoptosis of Retinoblastoma Cells via Inhibition of FOXG1.Invest Ophthalmol Vis Sci. 2020 May 11;61(5):31. doi: 10.1167/iovs.61.5.31. Invest Ophthalmol Vis Sci. 2020. PMID: 32428232 Free PMC article.
-
Green Light-Triggered Intraocular Drug Release for Intravenous Chemotherapy of Retinoblastoma.Adv Sci (Weinh). 2021 Oct;8(20):e2101754. doi: 10.1002/advs.202101754. Epub 2021 Aug 27. Adv Sci (Weinh). 2021. PMID: 34448360 Free PMC article.
-
USP14 increases the sensitivity of retinoblastoma to cisplatin by mediating the ferroptosis.Naunyn Schmiedebergs Arch Pharmacol. 2024 Nov;397(11):8671-8680. doi: 10.1007/s00210-024-03174-9. Epub 2024 May 31. Naunyn Schmiedebergs Arch Pharmacol. 2024. PMID: 38819674 Free PMC article.
References
-
- Chintagumpala M, Chevez-Barrios P, Paysse EA, Plon SE, Hurwitz R. Retinoblastoma: Review of Current Management. The Oncologist. 2007;12:1237–1246. - PubMed
-
- Shields JA, Shields CL. Treatment of Retinoblastoma with Photocoagulation. Trans. Pa. Acad. Ophthalmol. Otolaryngol. 1990;42:951–954. - PubMed
-
- Shields JA, Shields CL, De Potter P. Photocoagulation of Retinoblastoma. Int. Opthalmol. Clin. 1993;33:95–99. - PubMed
-
- Shields CL, Santos CM, Diniz W, Gündüz K, Mercado G, Cater JR, Shields JA. Thermotherapy for Retinoblastoma. Arch. Ophthalmol. 1999;117:885–893. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
