

Pulmonary-renal syndromes: Experience from an Indian Intensive Care Unit
- PMID: 26195857
- PMCID: PMC4478672
- DOI: 10.4103/0972-5229.158261
Pulmonary-renal syndromes: Experience from an Indian Intensive Care Unit
Abstract
Background: The etiology of patients presenting with pulmonary-renal syndrome (PRS) to Intensive Care Units (ICUs) in India is not previously reported.
Aims: The aim was to describe the prevalence, etiology, clinical manifestations, and outcomes of PRS in an Indian ICU and identify variables that differentiate immunologic causes of PRS from tropical syndromes presenting with PRS.
Materials and methods: We conducted a prospective observational study of all patients presenting with PRS over 1-year. Clinical characteristics of patients with "definite PRS" were compared with those with "PRS mimics".
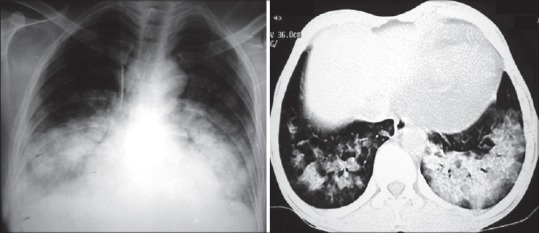
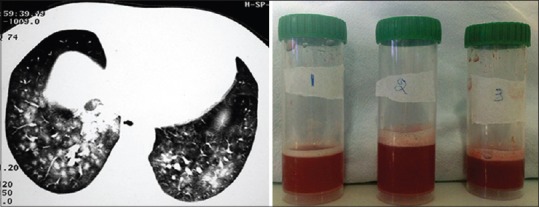
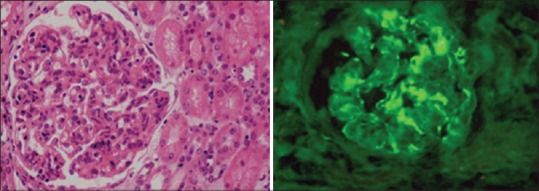
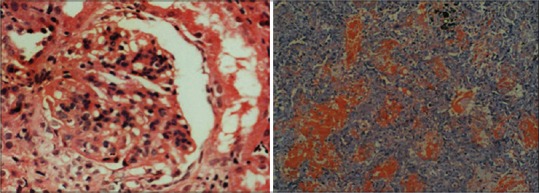
Results: We saw 27 patients with "provisional PRS" over the said duration; this included 13 patients with "definite PRS" and 14 with "PRS mimics". The clinical symptoms were similar, but patients with PRS were younger and presented with longer symptom duration. Ninety-two percent of the PRS cohort required mechanical ventilation, 77% required vasopressors and 61.5% required dialysis within 48 h of ICU admission. The etiologic diagnosis of PRS was made after ICU admission in 61.5%. Systemic lupus erythrematosus (54%) was the most common diagnosis. A combination of biopsy and serology was needed in the majority (69%, 9/13). Pulse methylprednisolone (92%) and cyclophosphamide (61.5%) was the most common protocol employed. Patients with PRS had more alveolar hemorrhage, hypoxemia and higher mortality (69%) when compared to "PRS mimics".
Conclusion: The spectrum of PRS is different in the tropics and tropical syndromes presenting with PRS are not uncommon. Multicentric studies are needed to further characterize the burden, etiology, treatment protocols, and outcomes of PRS in India.
Keywords: Crescentic glomerulonephritis; diffuse alveolar hemorrhage; pulmonary-renal; rapidly progressive renal failure; systemic lupus erythrematosus.
Figures

Similar articles
-
Pulmonary-Renal Syndrome: A Real-World Experience From a Tertiary Care Pulmonary Center in North India.Cureus. 2022 Jan 17;14(1):e21327. doi: 10.7759/cureus.21327. eCollection 2022 Jan. Cureus. 2022. PMID: 35186586 Free PMC article.
-
Pulmonary Renal Syndrome: Experience from Tertiary Centre in Mumbai.J Assoc Physicians India. 2018 Jul;66(7):13-17. J Assoc Physicians India. 2018. PMID: 31325253
-
[Pulmonary-renal syndromes].G Ital Nefrol. 2011 Jan-Feb;28(1):57-63. G Ital Nefrol. 2011. PMID: 21341246 Italian.
-
Diffuse alveolar hemorrhage in IgA nephropathy: case series and systematic review of the literature.Int J Rheum Dis. 2017 Jan;20(1):109-121. doi: 10.1111/1756-185X.12818. Epub 2016 Feb 4. Int J Rheum Dis. 2017. PMID: 26845236 Review.
-
[Goodpasture's syndrome--disease of many faces].Przegl Lek. 2013;70(4):218-23. Przegl Lek. 2013. PMID: 23991562 Review. Polish.
Cited by
-
Infection in systemic lupus erythematosus-associated diffuse alveolar hemorrhage: a potential key to improve outcomes.Clin Rheumatol. 2023 Jun;42(6):1573-1584. doi: 10.1007/s10067-023-06517-8. Epub 2023 Feb 17. Clin Rheumatol. 2023. PMID: 36797549
-
Pulmonary-Renal Syndrome: A Real-World Experience From a Tertiary Care Pulmonary Center in North India.Cureus. 2022 Jan 17;14(1):e21327. doi: 10.7759/cureus.21327. eCollection 2022 Jan. Cureus. 2022. PMID: 35186586 Free PMC article.
References
-
- Goodpasture E. The significance of certain pulmonary lesions in relation to the etiology of influenza. Am J Med Sci. 1919;158:863–70. - PubMed
-
- Nath A, Rajagopala S. Pulmonary renal syndromes: A pulmonologist's view. [Last accessed on 2015 May 15];Clin Queries Nephrol. 2015 4:1–10. doi:10.1016/j.cqn.2015.02.001.
-
- West SC, Arulkumaran N, Ind PW, Pusey CD. Pulmonary-renal syndrome: A life threatening but treatable condition. Postgrad Med J. 2013;89:274–83. - PubMed
-
- Gallagher H, Kwan JT, Jayne DR. Pulmonary renal syndrome: A 4-year, single-center experience. Am J Kidney Dis. 2002;39:42–7. - PubMed
-
- Rodriguez W, Hanania N, Guy E, Guntupalli J. Pulmonary-renal syndromes in the intensive care unit. Crit Care Clin. 2002;18:881–95. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources