

Genetic architecture of colorectal cancer
- PMID: 26187503
- PMCID: PMC4567512
- DOI: 10.1136/gutjnl-2013-306705
Genetic architecture of colorectal cancer
Abstract
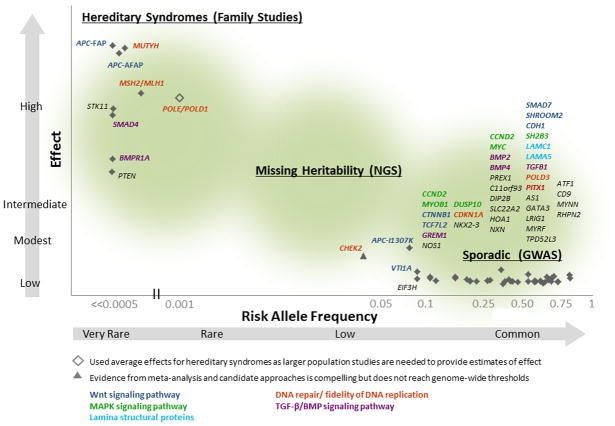
Colorectal cancer (CRC) is a complex disease that develops as a consequence of both genetic and environmental risk factors. A small proportion (3-5%) of cases arise from hereditary syndromes predisposing to early onset CRC as a result of mutations in over a dozen well defined genes. In contrast, CRC is predominantly a late onset 'sporadic' disease, developing in individuals with no obvious hereditary syndrome. In recent years, genome wide association studies have discovered that over 40 genetic regions are associated with weak effects on sporadic CRC, and it has been estimated that increasingly large genome wide scans will identify many additional novel genetic regions. Subsequent experimental validations have identified the causally related variant(s) in a limited number of these genetic regions. Further biological insight could be obtained through ethnically diverse study populations, larger genetic sequencing studies and development of higher throughput functional experiments. Along with inherited variation, integration of the tumour genome may shed light on the carcinogenic processes in CRC. In addition to summarising the genetic architecture of CRC, this review discusses genetic factors that modify environmental predictors of CRC, as well as examples of how genetic insight has improved clinical surveillance, prevention and treatment strategies. In summary, substantial progress has been made in uncovering the genetic architecture of CRC, and continued research efforts are expected to identify additional genetic risk factors that further our biological understanding of this disease. Subsequently these new insights will lead to improved treatment and prevention of colorectal cancer.
Keywords: COLORECTAL CANCER.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
The authors have no competing interests to disclose.
Figures

Similar articles
-
Genetic predisposition to colorectal cancer: where we stand and future perspectives.World J Gastroenterol. 2014 Aug 7;20(29):9828-49. doi: 10.3748/wjg.v20.i29.9828. World J Gastroenterol. 2014. PMID: 25110415 Free PMC article. Review.
-
Update on genetic predisposition to colorectal cancer and polyposis.Mol Aspects Med. 2019 Oct;69:10-26. doi: 10.1016/j.mam.2019.03.001. Epub 2019 Mar 18. Mol Aspects Med. 2019. PMID: 30862463 Review.
-
Diagnosing hereditary colorectal cancer.Clin Colorectal Cancer. 2010 Oct;9(4):205-11. doi: 10.3816/CCC.2010.n.030. Clin Colorectal Cancer. 2010. PMID: 20920991 Review.
-
Genetic variations in colorectal cancer risk and clinical outcome.World J Gastroenterol. 2014 Apr 21;20(15):4167-77. doi: 10.3748/wjg.v20.i15.4167. World J Gastroenterol. 2014. PMID: 24764655 Free PMC article. Review.
-
New genes emerging for colorectal cancer predisposition.World J Gastroenterol. 2014 Feb 28;20(8):1961-71. doi: 10.3748/wjg.v20.i8.1961. World J Gastroenterol. 2014. PMID: 24587672 Free PMC article. Review.
Cited by
-
Germline mutational profile of Chinese patients under 70 years old with colorectal cancer.Cancer Commun (Lond). 2020 Nov;40(11):620-632. doi: 10.1002/cac2.12093. Epub 2020 Sep 10. Cancer Commun (Lond). 2020. PMID: 32914570 Free PMC article.
-
Vitamin D and colorectal cancer: molecular, epidemiological and clinical evidence.Br J Nutr. 2016 May;115(9):1643-60. doi: 10.1017/S0007114516000696. Br J Nutr. 2016. PMID: 27245104 Free PMC article. Review.
-
Alterations of Gut Mycobiota Profiles in Adenoma and Colorectal Cancer.Front Cell Infect Microbiol. 2022 Feb 24;12:839435. doi: 10.3389/fcimb.2022.839435. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 35281451 Free PMC article.
-
Elevated G-Protein Receptor 125 (GPR125) Expression Predicts Good Outcomes in Colorectal Cancer and Inhibits Wnt/β-Catenin Signaling Pathway.Med Sci Monit. 2018 Sep 19;24:6608-6616. doi: 10.12659/MSM.910105. Med Sci Monit. 2018. PMID: 30231258 Free PMC article.
-
The Largest Chinese Cohort Study Indicates Homologous Recombination Pathway Gene Mutations as Another Major Genetic Risk Factor for Colorectal Cancer with Heterogeneous Clinical Phenotypes.Research (Wash D C). 2023 Oct 17;6:0249. doi: 10.34133/research.0249. eCollection 2023. Research (Wash D C). 2023. PMID: 37854294 Free PMC article.
References
-
- Ferlay J, Shin HR, Bray F, et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127(12):2893–917. - PubMed
-
- Howlader N, Noone A, Krapcho M, et al. In: SEER Cancer Statistics Review, 1975–2010. Cronin KA, editor. Bethesda, MD: National Cancer Institute; 2014. based on November 2012 SEER data submission, posted to the SEER web site, April 2013.
-
- Ferlay J, Soerjomataram I, Ervik M, et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11. Lyon, France: International Agency for Research on Cancer; 2013. [accessed on 12/06/2014]. http://globocan.iarc.fr.
-
- Lichtenstein P, Holm NV, Verkasalo PK, et al. Environmental and heritable factors in the causation of cancer--analyses of cohorts of twins from Sweden, Denmark, and Finland. N Engl J Med. 2000;343(2):78–85. - PubMed
-
- Czene K, Lichtenstein P, Hemminki K. Environmental and heritable causes of cancer among 9. 6 million individuals in the Swedish Family-Cancer Database. Int J Cancer. 2002;99(2):260–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical