

Dendritic Cell-Based Immunotherapy Treatment for Glioblastoma Multiforme
- PMID: 26167495
- PMCID: PMC4488155
- DOI: 10.1155/2015/717530
Dendritic Cell-Based Immunotherapy Treatment for Glioblastoma Multiforme
Abstract
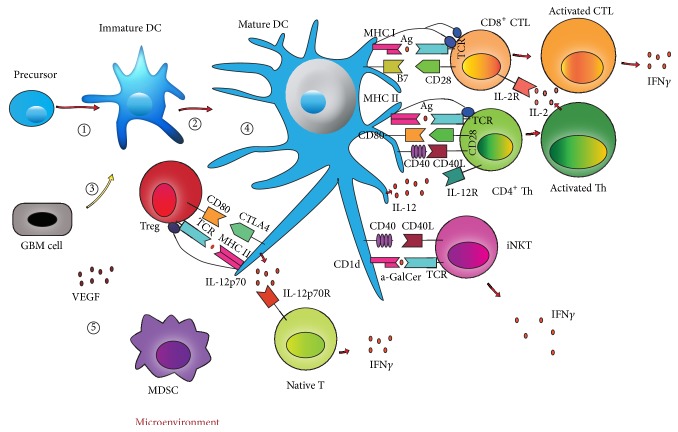
Glioblastoma multiforme (GBM) is the most malignant glioma and patients diagnosed with this disease had poor outcomes even treated with the combination of conventional treatment (surgery, chemotherapy, and radiation). Dendritic cells (DCs) are the most powerful antigen presenting cells and DC-based vaccination has the potential to target and eliminate GBM cells and enhance the responses of these cells to the existing therapies with minimal damage to the healthy tissues around them. It can enhance recognition of GBM cells by the patients' immune system and activate vast, potent, and long-lasting immune reactions to eliminate them. Therefore, this therapy can prolong the survival of GBM patients and has wide and bright future in the treatment of GBM. Also, the efficacy of this therapy can be strengthened in several ways at some degree: the manipulation of immune regulatory components or costimulatory molecules on DCs; the appropriate choices of antigens for loading to enhance the effectiveness of the therapy; regulation of positive regulators or negative regulators in GBM microenvironment.
Figures
Similar articles
-
Immunological analysis of phase II glioblastoma dendritic cell vaccine (Audencel) trial: immune system characteristics influence outcome and Audencel up-regulates Th1-related immunovariables.Acta Neuropathol Commun. 2018 Dec 5;6(1):135. doi: 10.1186/s40478-018-0621-2. Acta Neuropathol Commun. 2018. PMID: 30518425 Free PMC article. Clinical Trial.
-
Active immunotherapy using dendritic cells in the treatment of glioblastoma multiforme.Cancer Treat Rev. 2013 Dec;39(8):891-907. doi: 10.1016/j.ctrv.2013.05.007. Epub 2013 Jun 21. Cancer Treat Rev. 2013. PMID: 23790634 Review.
-
Treatment of a patient by vaccination with autologous dendritic cells pulsed with allogeneic major histocompatibility complex class I-matched tumor peptides. Case Report.Neurosurg Focus. 2000 Dec 15;9(6):e8. doi: 10.3171/foc.2000.9.6.9. Neurosurg Focus. 2000. PMID: 16817691
-
A randomized controlled phase II trial of vaccination with lysate-loaded, mature dendritic cells integrated into standard radiochemotherapy of newly diagnosed glioblastoma (GlioVax): study protocol for a randomized controlled trial.Trials. 2018 May 25;19(1):293. doi: 10.1186/s13063-018-2659-7. Trials. 2018. PMID: 29801515 Free PMC article.
-
DCVax-Brain and DC vaccines in the treatment of GBM.Expert Opin Investig Drugs. 2009 Apr;18(4):509-19. doi: 10.1517/13543780902841951. Expert Opin Investig Drugs. 2009. PMID: 19335279 Review.
Cited by
-
The Emerging Role of Myeloid-Derived Suppressor Cells in the Glioma Immune Suppressive Microenvironment.Front Immunol. 2020 Apr 24;11:737. doi: 10.3389/fimmu.2020.00737. eCollection 2020. Front Immunol. 2020. PMID: 32391020 Free PMC article. Review.
-
Development of bioactive materials for glioblastoma therapy.Bioact Mater. 2016 Apr 23;1(1):29-38. doi: 10.1016/j.bioactmat.2016.03.003. eCollection 2016 Sep. Bioact Mater. 2016. PMID: 29744393 Free PMC article. Review.
-
Tumor-Treating Fields for the treatment of glioblastoma: a systematic review and meta-analysis.Neurooncol Pract. 2021 Apr 20;8(4):426-440. doi: 10.1093/nop/npab026. eCollection 2021 Aug. Neurooncol Pract. 2021. PMID: 34277021 Free PMC article. Review.
-
The immune regulation of BCL3 in glioblastoma with mutated IDH1.Aging (Albany NY). 2022 Apr 29;14(9):3856-3873. doi: 10.18632/aging.204048. Epub 2022 Apr 29. Aging (Albany NY). 2022. PMID: 35488886 Free PMC article.
-
Construction and Validation of an Immune-Related Risk Score Model for Survival Prediction in Glioblastoma.Front Neurol. 2022 Mar 16;13:832944. doi: 10.3389/fneur.2022.832944. eCollection 2022. Front Neurol. 2022. PMID: 35370869 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
