

Cytomegalovirus infection in renal transplantation: clinical aspects, management and the perspectives
- PMID: 25993081
- PMCID: PMC4946822
- DOI: 10.1590/S1679-45082015RW3175
Cytomegalovirus infection in renal transplantation: clinical aspects, management and the perspectives
Abstract
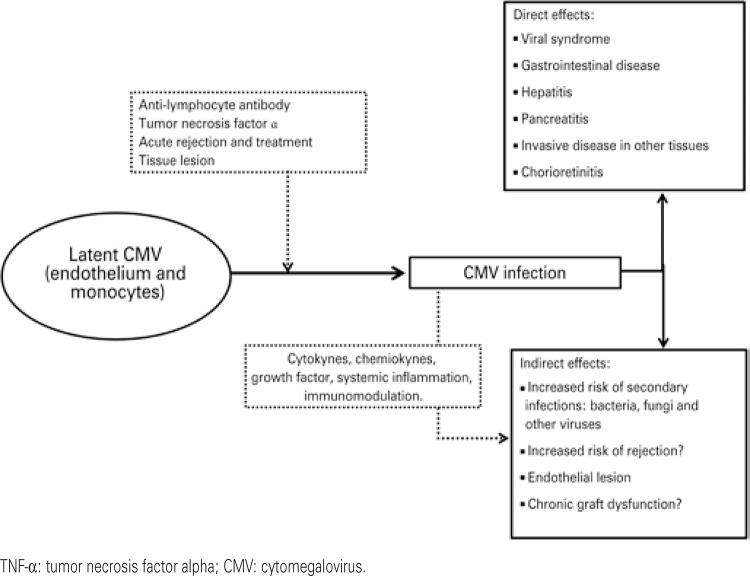
Cytomegalovirus infection is one of most frequent infectious complications after renal transplantation, and can be classified as primo-infection, when the transmission occurs through the graft, or reactivation, when the recipient is cytomegalovirus seropositive. After transplantation, cytomegalovirus can appear as an infection, when the patient presents with evidence of viral replication without symptoms or disease, which has two clinical spectra: typical viral syndrome or invasive disease, which is a less common form. Their effects can be classified as direct, while the disease is developed, or indirect, with an increase of acute rejection and chronic allograft dysfunction risks. Diagnosis must be made based on viremia by one of the standardized methods: antigenemia or PCR, which is more sensitive. The risk factors related to infection after transplantation are the serologic matching (positive donor and negative recipient) and anti-lymphocyte antibody drugs. One of the strategies to reduce risk of disease should be chosen for patients at high risk: preemptive treatment or universal prophylaxis. Recent clinical research has described ganciclovir resistance as an emergent problem in management of cytomegalovirus infection. Two types of mutation that cause resistance were described: UL97 (most frequent) and UL54. Today, sophisticated methods of immunologic monitoring to detect specific T-cell clones against cytomegalovirus are used in clinical practice to improve the management of high-risk patients after renal transplantation.
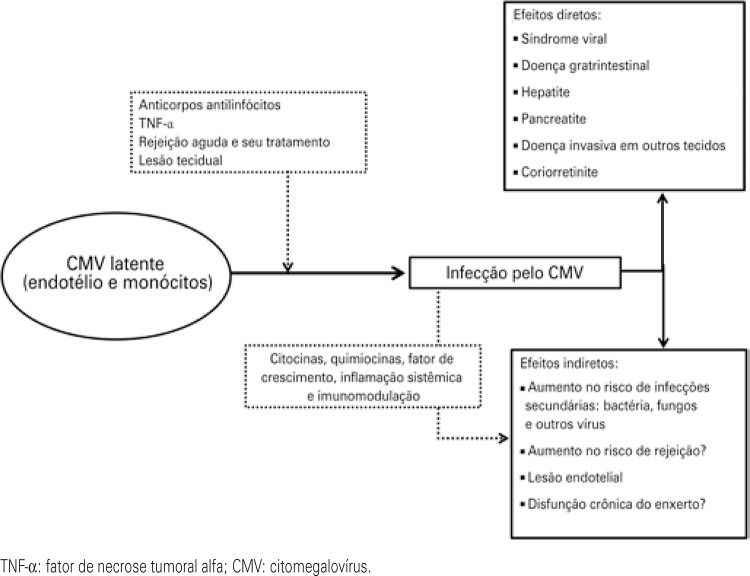
A infecção pelo citomegalovírus é uma das principais complicações após o transplante de rim, podendo ser classificada em primoinfecção, quando a transmissão ocorre por meio do enxerto, ou em reativação, quando o receptor é soropositivo. Do ponto de vista clínico, pode se apresentar como infecção, na ausência de sintomas, ou como doença, com dois diferentes espectros: a síndrome viral típica ou, menos comumente, a doença invasiva. Os efeitos podem ser diretos, que é o desenvolvimento da doença, ou indiretos, como aumento no risco de rejeição aguda e de disfunção crônica do enxerto. O diagnóstico deve ser feito por pesquisa de viremia por meio de um dos dois métodos padronizados: antigenemia ou PCR − sendo essa última a mais sensível. Os fatores de risco relacionados com a infecção após o transplante são o match sorológico (doador positivo e receptor negativo) e o uso de anticorpos antilinfócitos. Uma das estratégias de redução de risco de doença deve ser escolhida após o transplante nos pacientes de alto risco: tratamento preemptivo ou profilaxia. Recentemente, linhas de pesquisa clínica têm apontado a resistência ao ganciclovir como um problema emergente no manejo da infecção pelo citomegalovírus. Duas formas de mutação que causam resistência são descritas: UL97, que é a mais frequente, e a UL54. Atualmente, sofisticados métodos de monitorização imunológica, como a detecção de clones específicos de células T contra o citomegalovírus podem ser utilizados na prática clínica para o melhor manejo após o transplante renal dos pacientes de alto risco.
Figures
Similar articles
-
Reassessing the impact of cytomegalovirus infection in kidney and kidney-pancreas transplantation.Am J Kidney Dis. 2002 May;39(5):1088-95. doi: 10.1053/ajkd.2002.32793. Am J Kidney Dis. 2002. PMID: 11979354
-
The pathogenesis and clinical management of cytomegalovirus infection in the organ transplant recipient: the end of the 'silo hypothesis'.Curr Opin Infect Dis. 2007 Aug;20(4):399-407. doi: 10.1097/QCO.0b013e328285a358. Curr Opin Infect Dis. 2007. PMID: 17609600 Review.
-
[Effectiveness of preemptive therapy with ganciclovir in recipients of renal transplants at high risk (R-/D+) for the development of cytomegalovirus disease].Rev Invest Clin. 2002 May-Jun;54(3):198-203. Rev Invest Clin. 2002. PMID: 12183888 Spanish.
-
[Cytomegalovirus infection after solid-organ transplantation, its risk factors, direct and indirect effects and prevention strategies].Orv Hetil. 2008 Mar 23;149(12):551-8. doi: 10.1556/OH.2008.28324. Orv Hetil. 2008. PMID: 18343771 Review. Hungarian.
-
Cytomegalovirus in transplantation - challenging the status quo.Clin Transplant. 2007 Mar-Apr;21(2):149-58. doi: 10.1111/j.1399-0012.2006.00618.x. Clin Transplant. 2007. PMID: 17425738 Review.
Cited by
-
Torque Teno Virus: A Promising Biomarker in Kidney Transplant Recipients.Int J Mol Sci. 2024 Jul 15;25(14):7744. doi: 10.3390/ijms25147744. Int J Mol Sci. 2024. PMID: 39062987 Free PMC article.
-
The pattern of cytomegalovirus replication in post-renal transplant recipients with pre-emptive therapy strategy during the 1st year of post-transplantation.Int J Health Sci (Qassim). 2023 Sep-Oct;17(5):39-44. Int J Health Sci (Qassim). 2023. PMID: 37692991 Free PMC article.
-
Cytomegalovirus Induced Collapsing Glomerulopathy and Necrotizing Glomerulonephritis in a Renal Allograft Recipient.Indian J Nephrol. 2019 Mar-Apr;29(2):122-124. doi: 10.4103/ijn.IJN_375_17. Indian J Nephrol. 2019. PMID: 30983753 Free PMC article.
-
Association Between Cytomegalovirus Reactivation and Clinical Outcomes in Immunocompetent Critically Ill Patients: A Systematic Review and Meta-Analysis.Open Forum Infect Dis. 2017 Feb 13;4(2):ofx029. doi: 10.1093/ofid/ofx029. eCollection 2017 Spring. Open Forum Infect Dis. 2017. PMID: 29497626 Free PMC article.
-
Neurologic complications of kidney transplantation.Transl Androl Urol. 2019 Apr;8(2):164-172. doi: 10.21037/tau.2018.08.11. Transl Androl Urol. 2019. PMID: 31080777 Free PMC article. Review.
References
-
- Pass FR. Epidemiology and transmission of cytomegalovirus. J Infect Dis. 1985;152(2):243–248. Review. - PubMed
-
- Brennan DC. Cytomegalovirus in renal transplantation. J Am Soc Nephrol. 2001;12(4):848–855. Review. - PubMed
-
- Humar A, Snydeman D, AST Infectiuos Diseases Community of Pratice Cytomegalovirus in solid organ transplant recipients. Am J Transplant. 2009;9(Suppl 4):S78–S86. - PubMed
-
- Kasiske BL, Zeier MG, Chapman JR, Craig JC, Ekberg H, Garvey CA, Green MD, Jha V, Josephson MA, Kiberd BA, Kreis HA, McDonald RA, Newmann JM, Obrador GT, Vincenti FG, Cheung M, Earley A, Raman G, Abariga S, Wagner M, Balk EM. Kidney Disease: Improving Global Outcomes. Clinical practice guideline for the care of kidney transplant recipients: a summary. Kidney International. 2010;77(4):299–311. - PubMed
-
- Kuo HT, Ye X, Sampaio MS, Reddy P, Bunnapradist S. Cytomegalovirus serostatus pairing and deceased donor kidney transplant outcomes in adult recipients with antiviral prophylaxis. Transplantation. 2010;90(10):1091–1098. - PubMed
